






(Yes! Deltadave is in the house!) (I was hoping the whole "dial-winging" thing might help get him to post. )
(Now if we can just figure out a way to lure in -SWS.)
National (U.S.) Sleep Clinic Recommendations
Re: National (U.S.) Sleep Clinic Recommendations
DD,deltadave wrote:
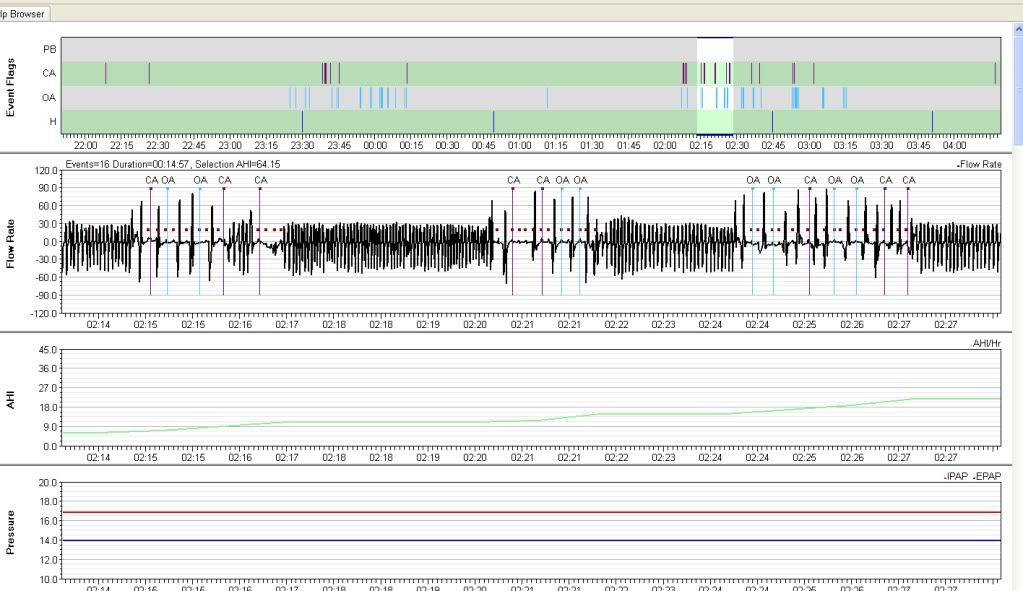
"IMHO", the software is claiming the events to be frank obstructive apnea vs flow limitation)(which might also be a subject of debate/discussion-- are they really obstructives? That certainly seems contrary to the information presented thus far).
I just want to confirm that you're talking about the PR/Sleepyhead software and not the software used during the sleep study - Correct?
I always was suspicious that these events (which make up the bulk of my events) could just as well be central in which case this would be a whole different game - correct?
I suppose that if I had a central and partially closed my throat and/or glottis then the machine could record them as obstructive (which it does) but occasionally (but not often) flags them as centrals....I wonder if a Res Med machine would see them differently?
Out of my 3 PR System Ones I own the Bi-PAP tags these type events with highest percentage of centrals. The straight CPAP almost ALWAYS sees them as obstructives. I wonder if the lower exhale pressure affects my throat/glottis or just the feedback on the pulse? It looks like the pulse feedbacks are borderline and sometimes it tags them as obstructives and sometime it tags them as centrals.
So what should I do from here?
Reason for editing: brain fog

Re: National (U.S.) Sleep Clinic Recommendations
Correct.Tom W wrote:I just want to confirm that you're talking about the PR/Sleepyhead software and not the software used during the sleep study - Correct?deltadave wrote:"IMHO", the software is claiming the events to be frank obstructive apnea vs flow limitation)(which might also be a subject of debate/discussion-- are they really obstructives? That certainly seems contrary to the information presented thus far).
In looking at the previously submitted data:
I would agree that there is a very strong possibility that they're ALL central.Tom W wrote:In the following flow patterns you can see both OA's and CA's that look pretty similarly shaped. I assume from the response of the pressure pulses that sometimes the airway is clear and sometimes it is closed. I'm beginning to think that perhaps the only difference is the position of my glottis. I don't really have any experience in this field besides trying to improve my own sleep but in these examples even the OA's seem to be central in nature. The apparent (to me) deliberate starting and stopping resembles a pattern of breath holding that I occasionally do during the day but obviously I can't hold my breath that long/often when awake. Just throwing some thoughts out for discussion. Feel free to tell me I'm wrong, crazy, etc..
Is it possible in the above examples of my airflow patterns that I'm awake?


Keeping in mind that if you did that during Wake in the sleep study, the events would not be noted whatsoever.
...other than food...
Re: National (U.S.) Sleep Clinic Recommendations
Confirm that supine REM is effectively being treated (it may very well be, cause it's unlikely that that's all supine REM there in Encore)(do you have the original diagnostic study?) and then start looking at sleep itself.Tom W wrote:So what should I do from here?
If all that "respiratory disturbance" is really "sleep disturbance" then fixing that would give you the biggest bang for the buck.
...other than food...
Re: National (U.S.) Sleep Clinic Recommendations
deltadave wrote:Confirm that supine REM is effectively being treated (it may very well be, cause it's unlikely that that's all supine REM there in Encore)(do you have the original diagnostic study?)Tom W wrote:So what should I do from here?
I requested copies of all my sleep studies from my original doctor yesterday.
Sorry, you lost me for a moment. Should I be looking to clear up the PLM's (which might help the sleep) or clearing up the apneas (which might clear up some of the PLM's and the sleep)?deltadave wrote:and then start looking at sleep itself.Tom W wrote:So what should I do from here?
If all that "respiratory disturbance" is really "sleep disturbance" then fixing that would give you the biggest bang for the buck.
Re: National (U.S.) Sleep Clinic Recommendations
Not for nothin', but the Sleep Study started and 8:32PM and finished at 3:46AM?
What's up with THAT?
What's up with THAT?
...other than food...
Re: National (U.S.) Sleep Clinic Recommendations
By that, are you referring to possible sleep-hygiene-related-type issues? Or am I misreading that? (If you mind my asking that about those words addressed to Tom.)deltadave wrote: . . . looking at sleep itself . . . "sleep disturbance" then fixing that . . .
Re: National (U.S.) Sleep Clinic Recommendations
I saw that too...I'm assuming it didn't take into account daylight savings time?deltadave wrote:Not for nothin', but the Sleep Study started and 8:32PM and finished at 3:46AM?
What's up with THAT?
I'd say it was more like 9:32 to 4:46.
Re: National (U.S.) Sleep Clinic Recommendations
Including all medications, caffeine intake, etc.jnk wrote:By that, are you referring to possible sleep-hygiene-related-type issues? Or am I misreading that? (If you mind my asking that about those words addressed to Tom.)deltadave wrote: . . . looking at sleep itself . . . "sleep disturbance" then fixing that . . .
That anemic REM needs some microanalysis.
...other than food...
Re: National (U.S.) Sleep Clinic Recommendations
Thanks.deltadave wrote:Including all medications, caffeine intake, etc.jnk wrote: . . . possible sleep-hygiene-related-type issues? . . .
That anemic REM needs some microanalysis.
Any thoughts on the likely/unlikely significance/nonsignificance of the NREM limb movements, or no? Red herring? Wrong tree to bark up? Insufficient data?

Re: National (U.S.) Sleep Clinic Recommendations
That is home video of me several years ago. I have video of me (not posted) when not on Mirapex and my movements then look more like the many other PLMD vids on YouTube, the movements are more contractions without the wild flailing. Multiple sleep studies have captured both the normal and the augmented movements, depending on where I was in their treatment. At this time my movements are consistent with normal PLMD movements. I don't know if the TENS Unit could have helped when augmentation was in play or not. Kinda doubt how effective anything could be against what is seen in the video.avi123 wrote:Question,kteague wrote:avi123 wrote:. (For the newbies who may not have seen my home video of what my augmentation looked like, the link is below. Ranks right up there with the embarassing mask pics. But I don't mind taking a hit for the team. lol)
Is it you doing the "augmentation" in the youtube piece?
_________________
| Mask: TAP PAP Nasal Pillow CPAP Mask with Improved Stability Mouthpiece |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Bleep/DreamPort for full nights, Tap Pap for shorter sessions |
My SleepDancing Video link https://www.youtube.com/watch?v=jE7WA_5c73c
Re: National (U.S.) Sleep Clinic Recommendations
Right now, I would say everything is still in play, and perhaps they are all contributors and interrelated.jnk wrote:Thanks.deltadave wrote:Including all medications, caffeine intake, etc.jnk wrote: . . . possible sleep-hygiene-related-type issues? . . .
That anemic REM needs some microanalysis.
Any thoughts on the likely/unlikely significance/nonsignificance of the NREM limb movements, or no? Red herring? Wrong tree to bark up? Insufficient data?
...other than food...
Re: National (U.S.) Sleep Clinic Recommendations
M-F up at 4:30deltadave wrote:Including all medications, caffeine intake, etc.jnk wrote:By that, are you referring to possible sleep-hygiene-related-type issues? Or am I misreading that? (If you mind my asking that about those words addressed to Tom.)deltadave wrote: . . . looking at sleep itself . . . "sleep disturbance" then fixing that . . .
That anemic REM needs some microanalysis.
2 cups of coffee first thing in the a.m.
1 hour commute
9-1/2 or 10 hours of work
1 hour commute
I carpool and when I'm NOT driving I try to stay awake on the way home but that's not always possible.
On the days that I drive I have one large cup of tea right before I leave for the ride home. The small amount of caffeine and having to use the restroom keeps me awake.
I settle down about an hour before bed. I'd like it to be more but it doesn't happen.
S-S usually up around 6:00
2-3 cups of coffee first thing in the a.m.
S-S evenings are down time with the family at home. There's a 50-50 chance of falling asleep watching TV before bed.
365:
Zyrtec, Singular, and Nasonex for allergies first thing in the a.m.
Occasionally Allegra-D (12 hour) if they're really bad..
No alcohol, No smoking, No Rec Drug use
Neither of my last sleep studies have shown any SWS but I guess that's not unusual when you're 50.
Sleepyhead average is just over 7 hours of sleep per night.
Re: National (U.S.) Sleep Clinic Recommendations
It's not unusual with limb movements.Tom W wrote: ...Neither of my last sleep studies have shown any SWS but I guess that's not unusual when you're 50.
_________________
| Mask: TAP PAP Nasal Pillow CPAP Mask with Improved Stability Mouthpiece |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Bleep/DreamPort for full nights, Tap Pap for shorter sessions |
My SleepDancing Video link https://www.youtube.com/watch?v=jE7WA_5c73c
Re: National (U.S.) Sleep Clinic Recommendations
For the newbie lurkers:
Drug stuff:
http://psych.fullerton.edu/mwhite/473pd ... 0Sleep.pdf
Hygiene stuff:
http://www.umm.edu/sleep/sleep_hyg.htm
Drug stuff:
http://psych.fullerton.edu/mwhite/473pd ... 0Sleep.pdf
Hygiene stuff:
http://www.umm.edu/sleep/sleep_hyg.htm