SleepingUgly wrote:If you have periods of dense events, and then periods of no/low events, I would wonder about positional apnea or REM-dependent OSA. But we can't tell that yet.
I've been thinking along those same lines, SU.
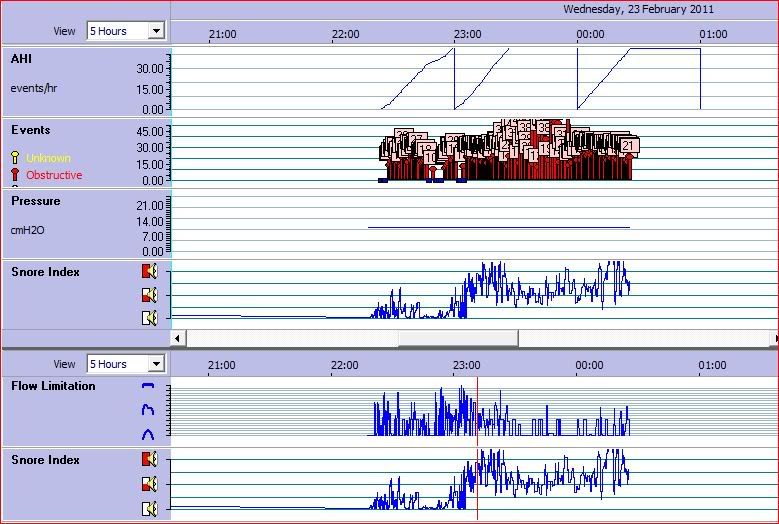
In this chart, I had noticed how the
duration of the apneas increased in the middle of the session, and wondered if that may be related to sleep position or REM. There are many 40-second apneas, and some are even longer because they go off the chart. It's very difficult to tell what's going on with such a limited number of hours. I'm not even sure when Alex is sleeping or awake. Things may look
quite a bit clearer when there are more hours recorded in one night, as sleep-cycle patterns will become more obvious.
There have been so many excellent suggestions here! To summarize, some things to consider are pressure adjustments, EPR, leak rate, and sleeping position. You are very fortunate to have found a mask that's comfortable, with few leaks! That's a big hurdle for most of us. Change things one at a time, so you know what works. It's generally recommended that you stay at one setting for a week or so since there can be nightly variation, but your case may be a little different since your treated AHI has been so high. Be sure to keep good records, recording things like pressure, EPR, mask used, sleep position, hours of use, AHI, AI (obstructive and any centrals), and leaks. It will be helpful to have this information as you tweak things.
Regarding sleep position, it can be very difficult to know whether you're rolling onto your back during the night. There are some ways to try to prevent that, such as filling a small backpack with something heavy or sewing a tennis ball(s) into the back of a tight shirt. There are a few commercial products too.
My own solution was cheap (free, actually). I made a homemade tennis ball setup to discourage myself from back sleeping. I cut a hole in the bottom of a tube sock, guided an old belt through the sock, put in two tennis balls, and secured the tennis balls in place with three rubber bands. I wore it wrapped around my
upper body, just under my armpits, with the tennis balls on my upper back. It may not work very well wearing this around your waist because it would fit into the small of your back. Effectiveness may also depend on how soft your mattress is.
Regarding machines, if your insurance bills by code (most do!), an APAP and a CPAP
do use the same billing code (E0601). That means that the insurance shouldn't care which machine you get. The DME may care because they make less profit on a CPAP. A doctor may care because he may want to see you more often (more money) and/or he is associated with a sleep center (more studies if you're not doing well). You may need to push the doctor/DME very hard for an APAP. Do that within the first 30 days. APAP should make self-titration easier, but you
can do it with a CPAP if you have to. Another thing, if insurance is involved they will have a minimum number of hours that you need to use the machine per night in order for them to continue to pay for it. That's another reason to work on increasing your mask time.
Alex, you're doing a
terrific job figuring this out! You have some of the most experienced people helping you on this thread, so you're in good hands. We are like family around here. But I hope you can develop a good relationship with your doctor too. I commend you for taking an active role in your therapy. It is absolutely
essential, especially in a case like yours. I'm also impressed that you have such a wonderful sense of humor and clarity of mind! I would be a cranky basket case.