Mr Bill wrote:Paper_Nanny wrote:
MSD talked to Bob, the Respironics Rep for much of the state of Oregon. Bob did in fact say I should be on a straight BiPAP, with no ASV. Why does this make sense? According to Bob, the the ASV is causing me to hyperventilate. That causes the CO2 level in my blood to go down, supressing the urge to breathe. When the CO2 level goes up, then I breathe. But, the ASV thinks I should be breathing sooner than that and triggers a breath. Thus, the PTB rate goes down after the first few hours of sleep.
Why does the ASV do that? Doesn't the algorithm figured out how fast I was breathing and time the breaths accordingly? According to Bob, that isn't quite right. The algorithm was deisgned for people with Cheyne-Stokes Respiration and CSA secondary to the use of opiods. It works great for people with that sort of SDB, but not for people like me.
OK, I am going to take a stab at explaining this from the existential participant point of view. This is the view where I try to extrapolate my existential relationship with my own ASV into the patterns I see you having.
First, I think ASV's like the patient to have a regular well spaced breathing pattern because they are designed to break up patterns of periodic breathing. So, if you have an erratic pattern of breaths due to your MS then the ASV will keep intervening to regularize the pattern.
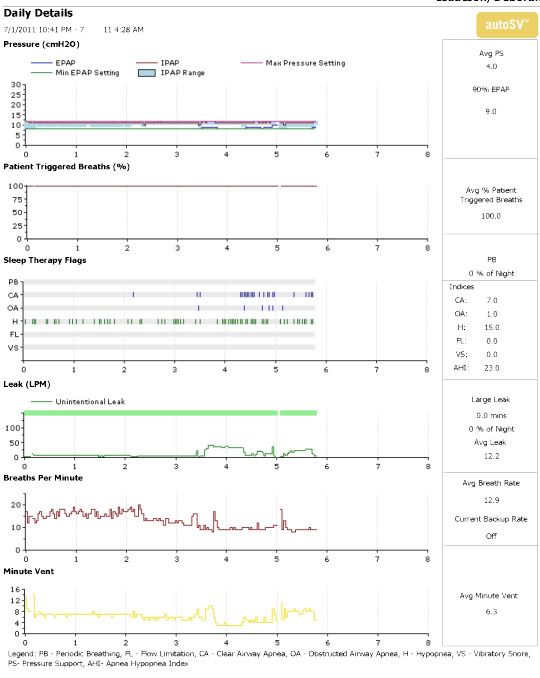
Second, Although the patient initiated breath graph looks horrible under full ASV control, I think probably, its not as bad as it appears. The ASV decides what your "breath timing slots" should be after measuring your average breath rate and tidal volume and probably some other timing and flow rate factors and I think it probably does some sort of predictive filtering sort of like a moving average to guess when the next breath should be.
Just because it nudges you to start a breath does not mean it pushes in the whole breath. I've noticed with mine that it starts the breath but it does not follow through come hell or high water unless, unless, I persist in not breathing, then the pressure ramps up. Now pressure can ramp up both to open the airway and to inflate lung. I'm not at all informed how much more pressure differential is needed to inflate the lungs if we just lay there like a dead fish. But my RT says an ASV will actually do it if set to have a backup rate.
So the patient initiated breath graph is probably a moving average. as the percentage drops with each "missed time slot". You may actually be doing 90% of the work even if you are doing 0% of the breath initiation. However, estimating that percentage of effort is probably not very easy or accurate outside of a lab. So, you see the Respironics rep is saying 'its not desirable but probably not harmful'. I suppose the only way to know for sure would be if the polysonmography could actually measure your exertion during sleep.
Third, it may be that you are having alpha wave intrusion (mild arousals while unconscious during sleep) because of these breath initiations which are making you feel less rested even though your AHI is looking pretty good.
Fourth, possibly you feel better with the recently tried BIPAP mode because you got to set your own breathing rhythm but the ASV logs every deviation from a steady train of pulses as hyponeas or clear airway apneas.
Fifth, its probably a good thing in the long run that the ASV tries to enforce a steady pattern of breaths no matter what causes breathing to be erratic. It took me months to get used to breathing 18 bpm when my natural rate is closer to 8. But I have gotten there and I keep sleeping better and better.
Now to the answer phase. I have to confess I wish I could sleep deeper most of the time. It has taken me 4 months to get over 4.5 hours a night and now my average after 7 months (just for the last 3 months) is 6.5 hours. But I can tell that I need to sleep deeper and longer. Its too easy to get woke up. I'll hazard that the ASV can treat your symptoms better than a BIPAP if the ASV could be adjusted to the widest possible leeway in breath variability. I believe somebody already mentioned that the inspiration time had to be less than 3 seconds to make the ASV happy. I wonder if setting your Inspiration time to the max would help? Also, since you have an average BPM of around 10 maybe setting a backup rate at 8 (ask Dr and RT if this is OK). On auto, maybe the unit is trying to speed you up to some default value. Finally, the rise time can be set higher, if I understand correctly, rise time is how quickly the ASV tries to bump up the pressure for an individual breath. Maybe if it is constrained to rise slowly, it will be less disturbing to your sleep as it tries to correct you to an even pattern. Lastly, I think you may start feeling more refreshed over time. I know my own experience after the first rush of getting sleep was to then realize for several months how much I needed it and how little I was getting. Maybe with time your sleeping mind will start accepting the ASV's nudges and not be aroused and then you will start really sleeping.
So, I'm not a medical doctor but I think you need the ASV in the long haul.
Edited for truth in advertising...












{kind=link}
{kind=link}
{kind=link}