







Of course I do! Why wouldn't I?deltadave wrote:Well do you know what means "ballistocardiographic"?NotMuffy wrote:I don't think so.deltadave wrote:I think he meant "WTF is 'ballistocardiographic?' "NotMuffy wrote:No, I'm sure the ones that are out there are OK.idamtnboy wrote:Are you expanding the definition of ballistocardiographic?
Otherwise, he would have simply asked, "WTF is 'ballistocardiographic?' "
Central Apneas and Respiratory Rate
Re: Central Apneas and Respiratory Rate
"Don't Blame Me...You Took the Red Pill..."

Re: Central Apneas and Respiratory Rate
OK then, use it in a sentence.NotMuffy wrote:Of course I do! Why wouldn't I?deltadave wrote:Well do you know what means "ballistocardiographic"?NotMuffy wrote:I don't think so.deltadave wrote:I think he meant "WTF is 'ballistocardiographic?' "NotMuffy wrote:No, I'm sure the ones that are out there are OK.
Otherwise, he would have simply asked, "WTF is 'ballistocardiographic?' "
...other than food...
Re: Central Apneas and Respiratory Rate
Well, in both of the above cases I believe machine-state theory would have RR calculations alternating between these two virtual machine states: state-1) calculating RR and state-2) waiting to calculate the next RR value. The event-trigger to transition from machine state-1 to machine state-2 would be a finalized RR calculation (that takes far less than any breath). And the event-trigger to transition from machine state-2 back to machine state-1 would be nothing more than either the "leading edge" or "trailing edge" of inhalation----since either inspiratory edge neatly delineates exactly one recurring breath period. And breath rate is really nothing more than a basic frequency calculation....idamtnboy wrote:The end result is the same.-SWS wrote: I don't understand the distinction. How would suspending or temporarily stopping any given update algorithmically differ from waiting to update? I'm formally trained in microprocessor algorithms and these two machine states sound equivalent to me.
...So counting the leading edges or trailing edges of inspiration is all we need---that and a real-time clock. Because calculating frequency (beath rate in this case) is always a matter of counting recurring periods and dividing by time. And the recurring inspiratory edges delineating each breathing period are pretty straight-forward to count: basically need an edge to count and a qualifying amplitude threshold or more sophisticated signal-noise filter.idamtnboy wrote:The way I'm thinking is that there are two separate routines, among many, running in the S9. One, the FAR, is looping at a frequency of 25 Hz. One of the data points it's looking for is when the flow rate hits zero on the upward move (actually some minor +/- value as it will almost never sample the flow rate exactly on the zero point). At that moment it sets a time mark. The next time it sees the zero point it sets the next time mark and calculates the time span. It then puts that time value on the stack. Since breaths are variable in length the new number can be put on the stack at any point in time, regardless of the elapsed time since the previous update.
At the same time we have the R3 loop running constantly at 0.5 Hz. It runs regardless of the state of the breath flow, and outputs the BPM # every two seconds.
When we have an apnea the flow stays near zero. I'm suggesting the FAR continues to run at 25 Hz. But it doesn't set a time mark because the conditions to do so are not met. The way I see it, suspend means the part of the FAR that is looking to set the time marks is stopped by some other command from outside of itself. Its frequency of looping drops to zero, hence it does not update the stack because it stops watching the flow rate and so has no new number with which to update the stack. "Spinning its wheels" means the part of the FAR that sets the time marks continues to sample the flow rate at 25 Hz, but it does not see the conditions required to set the time mark, so it does not have a number to put on the stack. Either way, the end result is the same, the BPM number stays stagnant because the data used to calculate it stays stagnant.
I would think that in all of the microprocessor routines you've been involved with some are designed to loop forever, never stopping except for loss of power, but only spit out a result when certain conditions they read are met. Others, on the other hand, check for some outside parameter, and if that parameter is at the correct state, the loop stops dead in its tracks. The second one is suspended or killed depending on whether or not it can be restarted by an outside parameter, the first one is not, but neither is updating its result. Now, if I have it wrong please set me straight. I have no direct microprocessor experience but am a little bit familiar with command languages, do loops, computer program routines, logic diagrams, etc.
The selected granularity toward algorithmic decision-making would be the designer's choice. And if that selected granularity is wider than unsuspecting human eyes expect, then they're going to wonder WHY RR doesn't drop to zero when flow plummets for 10 or 15 seconds... I would point out that the RR and volume graphs weren't offered as S9 graphs. Rather, we had to modify the software per gvz's excellent discovery, just to get them to print with S9 reports. I think the RR and volume graphs were REALLY designed for Resmed BiLevel machines. It wouldn't be all that tough for anyone to design an RR graph that drops to zero during an apnea----if there was a compelling design decision to do so IMHO.
Re: Central Apneas and Respiratory Rate
"You look very ballistocardiographic today."deltadave wrote:OK then, use it in a sentence.NotMuffy wrote:Of course I do! Why wouldn't I?deltadave wrote:Well do you know what means "ballistocardiographic"?NotMuffy wrote:I don't think so.deltadave wrote:I think he meant "WTF is 'ballistocardiographic?' "
Otherwise, he would have simply asked, "WTF is 'ballistocardiographic?' "
"Don't Blame Me...You Took the Red Pill..."
Re: Central Apneas and Respiratory Rate
Forensics needs another bullet and a beef heart to check ballistocardiographics from the assassin's gun...deltadave wrote: OK then, use it in a sentence.
I bet Dr. Rapoport knows.

Re: Central Apneas and Respiratory Rate
I concur completely. For example, in the case of an obstructive apnea, reporting an RR of zero would be erroneous. Respiratory efforts continue. It's flow that = 0.-SWS wrote:I think the RR and volume graphs were REALLY designed for Resmed BiLevel machines. It wouldn't be all that tough for anyone to design an RR graph that drops to zero during an apnea----if there was a compelling design decision to do so IMHO.
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem

Re: Central Apneas and Respiratory Rate
Maybe I shouldn't have ever enabled the RR graph in Resscan! Then I wouldn't have the curiosity to ask the question!
But this has been an interesting discussion, and since none of us, as far as has been disclosed, has inside knowledge of the S9 innards, we may all be right, or we may all be wrong, or we all may be part right and part wrong! Take your pick.
But this has been an interesting discussion, and since none of us, as far as has been disclosed, has inside knowledge of the S9 innards, we may all be right, or we may all be wrong, or we all may be part right and part wrong! Take your pick.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Hose management - rubber band tied to casement window crank handle! Hey, it works! S/W is 3.13, not 3.7 |
Re: Central Apneas and Respiratory Rate
I thought maybe the word would have been "ballistopulmonographic" since we're dealing with air, or is it hot air? After I post this I'll look to see if that word even exists.NotMuffy wrote:Of course I do! Why wouldn't I?deltadave wrote:Well do you know what means "ballistocardiographic"?NotMuffy wrote:I don't think so.deltadave wrote: I think he meant "WTF is 'ballistocardiographic?' "
Otherwise, he would have simply asked, "WTF is 'ballistocardiographic?' "
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Hose management - rubber band tied to casement window crank handle! Hey, it works! S/W is 3.13, not 3.7 |
Re: Central Apneas and Respiratory Rate
It does now! I just invented it! What it's definition? H***, I don't know! Just because I invent it doesn't mean I have to define it, right?idamtnboy wrote:I thought maybe the word would have been "ballistopulmonographic" since we're dealing with air, or is it hot air? After I post this I'll look to see if that word even exists.
OK, here's a definition:
That portion of the graphical depiction of the air flow during a breath cycle that looks like a failed missile shot, i.e., where it breaks out of the surface, goes up only a short way, wobbles around some, and then falls back to or under the surface.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Hose management - rubber band tied to casement window crank handle! Hey, it works! S/W is 3.13, not 3.7 |
Re: Central Apneas and Respiratory Rate
In this context, ballistocardiographic artifacts refer to "heartbeat pulsations" sitting in the flow channel as signal noise. They are also referred to as "cardiac oscillations" or "cardiogenic oscillations".NotMuffy wrote:
... and the ballistocardiographic artifact at 3A has contaminated the RR calculation.
Similarly, while respiratory rate should have slowed at Breath 6, another ballistocardiographic artifact at 5A (although without simultaneous EKG tracing, we can debate the the actual origin of the artifact) artificially maintains the high RR.
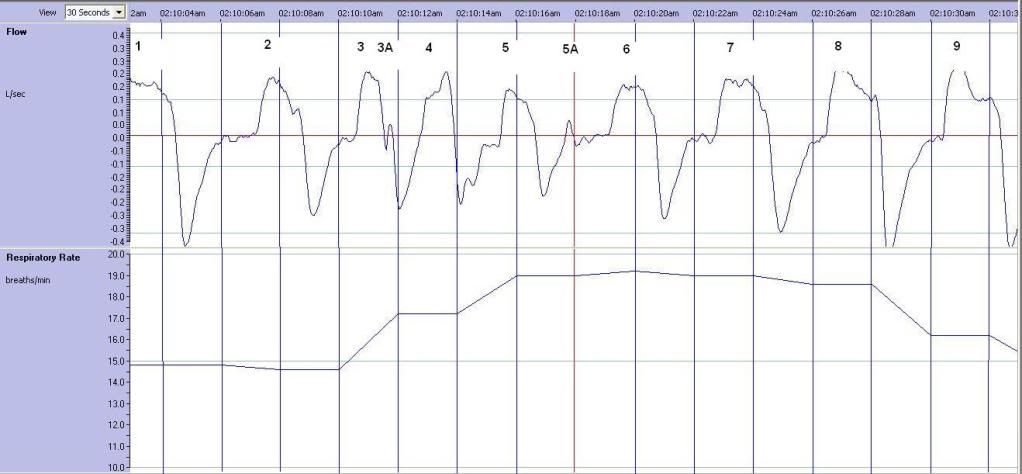
Dr. Rapoport, the 420e's designer, intentionally used those heartbeat signals (sitting in the flow channel) to differentiate central from obstructive apneas:
http://chestjournal.chestpubs.org/content/116/3/660
But in the S9 chart above, they appear to skew RR calculations as signal noise.
Re: Central Apneas and Respiratory Rate
Agreed. My understanding is that those might even be a few "inspiratory hitches" a.k.a. "false starts" during inhale. Respironics refers to them as such and even filters them out in at least one of their patent descriptions.NotMuffy wrote:although without simultaneous EKG tracing, we can debate the the actual origin of the artifact
In any event, I found myself wondering WHY the Resmed designers didn't take the extra steps to filter out those artifacts... Then I realized that occasionally being off-the-mark with RR+1 or even RR+2 would probably not significantly impact the treatment algorithms...
However, VPAP adaptSV---with its highly-responsive proportional-assist during IPAP---is undoubtedly Resmed's most real-time demanding treatment algorithm. And more program-execution steps to unnecessarily filter occasional RR artifacts could detract from the VPAP adaptSV's ability to deliver that necessary real-time responsiveness:

Hitting those proportionally-assisted set points at just the right moments requires real-time precision.
Re: Central Apneas and Respiratory Rate
It's almost unbelievable how sensitive an xPAP is when it comes to reading pressure. The idea that the pressure monitor in the machine can detect the pressure pulses in a moving air stream 6 to 7 feet down a hose resulting from the lung movement caused by heart beats, is astounding! At least I think so. I had no idea this was the case. That's why the cardio part of "ballistocardiographic" just didn't seem to fit the flow graph.
Several years ago when I was working for the Strategic Petroleum Reserve in Louisiana and Texas we explored the feasibility of detecting leaks in oil pipelines by monitoring the pressure in the pipeline. Looks like maybe the contractor who was trying to sell us a system should have hired some CPAP designers to work on the project! As it was, his proposed system failed to detect leaks in the line while oil was flowing.
Several years ago when I was working for the Strategic Petroleum Reserve in Louisiana and Texas we explored the feasibility of detecting leaks in oil pipelines by monitoring the pressure in the pipeline. Looks like maybe the contractor who was trying to sell us a system should have hired some CPAP designers to work on the project! As it was, his proposed system failed to detect leaks in the line while oil was flowing.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Hose management - rubber band tied to casement window crank handle! Hey, it works! S/W is 3.13, not 3.7 |
Re: Central Apneas and Respiratory Rate
Good save.idamtnboy wrote:It's almost unbelievable how sensitive an xPAP is when it comes to reading pressure. The idea that the pressure monitor in the machine can detect the pressure pulses in a moving air stream 6 to 7 feet down a hose resulting from the lung movement caused by heart beats, is astounding! At least I think so. I had no idea this was the case. That's why the cardio part of "ballistocardiographic" just didn't seem to fit the flow graph.
Since this is Lent, I won't say:
"Maybe if you opened your mind and shut your mouth, a lot more understanding would seep in."
As previously demonstrated, filtering "hides" (or sometimes "exposes") a great deal of data. Heart Rate Variability is especially interesting.
However, pulse wave technology is all around us, if you know where to look. Here is a graphic representation of an unfiltered, ultra low frequency, high amplitude waveform:
You Wanna See Astounding?
This also shows "turbulent" (as opposed to "laminar") flow patterns.
Imagine what a laminar flow pattern would have been like.
"Don't Blame Me...You Took the Red Pill..."
Re: Central Apneas and Respiratory Rate
Thank you.NotMuffy wrote: Good save.
I thought I did, eventually!! One of my bosses had a sign with a quote from I don't where, "The greatest impediment to finding a solution is already having the answer!"
Since this is Lent, I won't say:
"Maybe if you opened your mind and shut your mouth, a lot more understanding would seep in."
How often have we seen that, even in the medical profession? A doctor "just knows" a particular symptom means such and such disease, only to find out later the patient had an entirely different ailment. For example, my wife had serious back pain and surgery was being contemplated. Then her previously unknown stomach ulcer blew up. The back pain had been caused by the ulcer being in contact with the pancreas.
The tsunami monitoring and warning system is quite an accomplishment. I'm having difficulty visualizing what the difference would have been in that video between turbulent and laminar flow. Fluid mechanics was not one of my favorite subjects in college 45 years ago, and I mostly paid attention to laminar vs turbulent in terms of heat transfer at warm surfaces. Laminar flow contributes to plaque build up in arteries doesn't it?
As previously demonstrated, filtering "hides" (or sometimes "exposes") a great deal of data. Heart Rate Variability is especially interesting.
However, pulse wave technology is all around us, if you know where to look. Here is a graphic representation of an unfiltered, ultra low frequency, high amplitude waveform:
You Wanna See Astounding?
This also shows "turbulent" (as opposed to "laminar") flow patterns.
Imagine what a laminar flow pattern would have been like.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Hose management - rubber band tied to casement window crank handle! Hey, it works! S/W is 3.13, not 3.7 |

Re: Central Apneas and Respiratory Rate
Following this discussion brings to mind the digital signal processing class I had back in grad school. If one has a good idea of the shape of the signal one is looking for its pretty routine to be able to back that out of a string of data using Fourier transforms. We used to calculate FFT's for comparable amounts of data with our 7MHz 8086/8087 CPU's. So, if these higher end boxes have decent CPU's and a little storage I think its entirely possible they are getting heartbeat and pulse frequency events as well as breathing volume and frequency.
This whole thing has been on my mind quite a bit since I can visually see correlations between oxygen saturation and heart rate in the data from my pulse oximeter. I have been thinking about trying FFT on those by auto-correlating those two signals. But then what does one actually have?
This whole thing has been on my mind quite a bit since I can visually see correlations between oxygen saturation and heart rate in the data from my pulse oximeter. I have been thinking about trying FFT on those by auto-correlating those two signals. But then what does one actually have?
EPAP min=6, EPAP max=15, PS min=3, PS max=12, Max Pressure=30, Backup Rate=8 bpm, Flex=0, Rise Time=1,
90% EPAP=7.0, Avg PS=4.0, Avg bpm 18.3, Avg Min vent 9.2 Lpm, Avg CA/OA/H/AHI = 0.1/0.1/2.1/2.3 ... updated 02/17/12
90% EPAP=7.0, Avg PS=4.0, Avg bpm 18.3, Avg Min vent 9.2 Lpm, Avg CA/OA/H/AHI = 0.1/0.1/2.1/2.3 ... updated 02/17/12