I think that atrial fibrillation (or flutter) in anyone (let alone a 39 year old) should not be considered a "normal" phenomenon.Casiesea wrote:Echo - Within normal limits - Left atrium contracting more frequently then the other chambers (having trouble keeping up with the rest of heart), however test results still considered normal. Probably related to sleep problems...
What do you all think?
Just goes to show ya, nothing gets by -SWS!-SWS wrote:President-elect Doc1...
You give yourself far too much credit.Banned wrote:My problem is I also don't mind messing with sleep medicine professionals
Wrong again. What is very clearly stated is thatBanned wrote:Example: The Adapt SV literature clearly states that an EEP of 8cmH2O and MIN PS of 5cmH2O is a good starting point for 90% of Adapt SV patients.
Start therapy at default settings.
ASV Mode default settings:
EEP = 5 cm H2O (EEP = EPAP)
Minimum Pressure Support (Min PS) = 3 cm H2O
Maximum Pressure Support (Max PS) = 10 cm H2O
SAG wold opine that "Doc #1" has chosen to order "off the menu" a bit. The AdaptSV titration did not show results at EEP 10 cmH2O:goose wrote:I would also be quite interested in what SAG would opine here!!
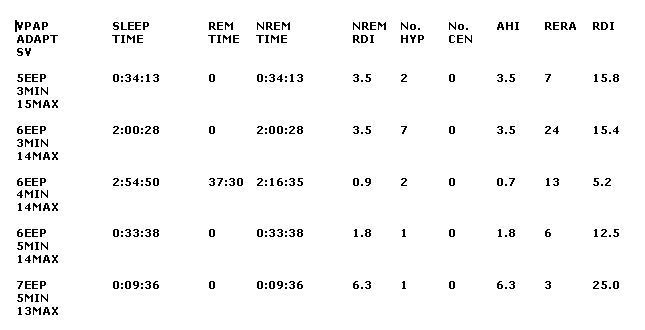
but they are opting to try that setting. However, since the titration showed that there continued to be obstructive events at the pressures trialed, then attempting to address them seems to be an appropriate course of action. The question would be whether you would want to address them by increasing EEP or by increasing PS. Increasing PS could be destabilizing to the CompSAS (let's say that CompSAS is present.) Might 10 cmH2O be a bit aggressive? Got me. They're there looking at the stuff.
Speaking of which, as everyone has noted (with the obvious exception of one poster), trying to understand things with snippets of information is difficult. Making treatment decisions is impossible.
As Lubman noted, they should be doing Adapt SV downloads and reviewing the data. There can be clues to treatment efficacy even if you're using the "unenhanced" AdaptSV.
SAG