Once again, -SWS, I come back to you with hat-in-one-hand and a Subway Thin-Sliced Crow Sandwich in the other.
You told me to think outside the box...
-SWS wrote:Absolutely no disrespect, sir... But that's what any subscriber to a biologically-mechanistic paradigm with a linear problem-solving approach might "have". I believe that type of paradigm and linear approach to be absolutely essential in science. However, it doesn't necessarily work well regarding exploration of a largely unknown behavioral/cognitive side of the autonomic sleep bridge. Rather, it politely says: "Everybody needs to get back on the biologically mechanistic side of the bridge and resume thinking inside the mechanistic box."
But
did I listen? Noooooooooooooooo..............
For over a hundred posts in this thread, and 20 years before this (I'm "somewhat" older than I look), I have said "Watch out for cardiac oscillations, they can really mess you up". Cause other than Rapoport, Norman, et al and the PB420E, nobody really got much benefit from looking at 'em.
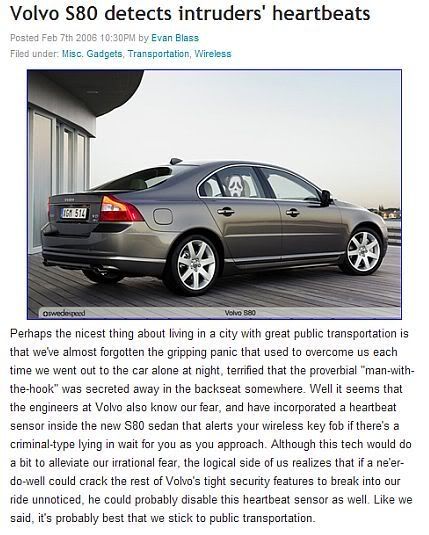
So last night, I sees this commercial where a young woman is walking out to her car in the middle of the night, all alone in a deserted parking lot. She looks at her electronic car key, sees a flashing red light and thinks to herself, "Aha!! Jack-the-Ripper is in the back seat of my car!!" and runs off to safety. (Course, one would have thought that maybe some other alarm would have sounded before that point, but that's the "scientific" me.)(Or better yet, a young woman walking out to her car in the middle of the night, all alone in a deserted parking lot, doesn't need an alarm system, she needs a lobotomy.)
So somebody took this:

...and, using this phenomenon (ballistocardiography) did this...
and now is probably a zillionaire.
Well, I'll show them! I am working on a system where, when cardiac oscillations are seen on a pressure transducer, an alarm will sound to alert the user that Jack-the-Ripper is on the other end of the CPAP machine.
Am I "out of the box" or what?
SAG










