






Oooh, I got a good shot of oscillations (not those specifically), post it when I get back.... kid thing...
SAG
Question on apap
-
StillAnotherGuest

- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
I Got That...

Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
So Them Lumps Is Cardiac Oscillations
OK great, I got an extra rake.ozij wrote:Ah, but our trees don't drop their leaves for winter the way yours do...
Y'know, when you blow those areas up, that's the only thing that would seem to make sense.ozij wrote:So, a "double tick apnea" is one which is central, but part of the time the machine is loosing the heartbeat and that's why it's adding the top tick?
Aha! Almost came to the Dark Side of "Not! Not! Not!"rested gal wrote:I've kept forgetting (for two years now!) to ask about something:StillAnotherGuest wrote:It's only 100% accurate (in a small study) in saying that the centrals it does find are centrals.
If the 420E is 100% accurate that when it says it saw a central, it really was a central, how come there was this...
Yeah, the actual waveform from 420E wasn't being looked at, so we'll never really know.
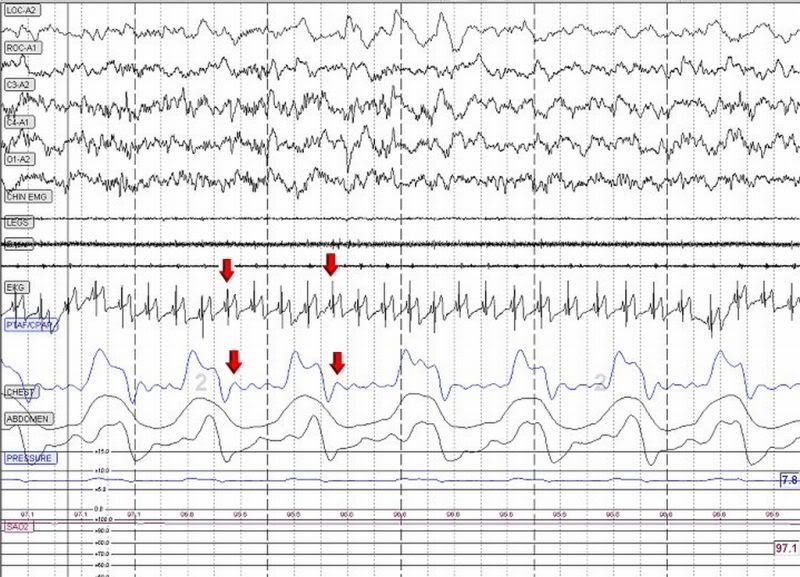
That Sensitivity/Specificity for the 420E centrals was a tiny study, so that 100% might be off. What it would take would be a patient with a fairly pronounced cardiac pulsation that would be sensed by 420E regardless of the airway state (including an obstructed airway). And you might just fit the bill. Although this is normal breathing, with the airway open, the cardiac pulsation is quite pronounced, just match up a QRS with the oscillation, there's even one stuck in a breath:
I'll have to go find that 420E "centrals" area to see if the pulsation appeared there, too, and if there's some sort of clue to document that concurrent event thing.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
I'll Take A Respiratory Event With Everything - To Go
On the other hand, trying to explain that simultaneous obstructive apnea/central apnea/hypopnea might be a little difficult.
SAG
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
Edging over a little closer to the Dark side...
I don't think I fit that bill, cuz that number of centrals happened only on that one night. Not before. Not after.What it would take would be a patient with a fairly pronounced cardiac pulsation that would be sensed by 420E regardless of the airway state (including an obstructed airway). And you might just fit the bill.
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Not THAT Bill..
No, the cardiac pulsations bill, not the centrals bill.
In other words, you could be the one who breaks out of the 100% specificity mold.
SAG
In other words, you could be the one who breaks out of the 100% specificity mold.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.

is there normally a pause between say an obstructive apnea and a post-arousal central?StillAnotherGuest wrote: On the other hand, trying to explain that simultaneous obstructive apnea/central apnea/hypopnea might be a little difficult.
For example; patient starts off with a hypopnea (10 sec, >50% flow), develops into a full apnea (>10sec, 0% flow) then is followed by a post-arousal central,
would that not produce the vertically aligned events you zoomed in on above?
I really don't know the duration of a "tic" on a 420e or time it represents, I would assume it is 10 seconds?
Since...
Flow limitation is reduction in air flow of <50% flow lasting 10 seconds or longer,
Hypopnea is reduction in flow of >50% lasting 10 seconds or longer in duration
Apnea is occluded or no flow.
My understanding is the 420e only scores CA's on line 2 when it hears cardiac oscillations associated with an open airway. So for the CA's found on line 2, it hears cardiac oscillations associated and is 100% accurate in those detections.
Next they cite in the help screens of a study that suggests only about 60% of central apnea is thought to be associated with an open airway, for the rest, the airway may be closed just as with a obstructive apnea (what the heck is the difference? respiratory effort?), in which case I would assume that the 420e would score those found with a closed airway (absence of cardiac oscillations) as plain ole obstructive apnea seen on line 1.
Weather or not it responds to an apnea seems to depend on 1) if cardiac oscillations are heard; 2. Command on Apnea settings and current pressure.
Still a great little machine with more features then some of the latest.
someday science will catch up to what I'm saying...
-
rested gal
- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
That's what I'm questioning..that 100% accuracy of the 420E in being correct - always correct - when it says "Now, THAT's a central apnea." I always thought the 420E would be right about that. Now I wonder.Snoredog wrote:My understanding is the 420e only scores CA's on line 2 when it hears cardiac oscillations associated with an open airway. So for the CA's found on line 2, it hears cardiac oscillations associated and is 100% accurate in those detections.
At the same time the 420E was chalking up those centrals for me, the PSG equipment was saying "centrals = zero."
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
to be honest, I really don't know where that "100% accuracy" claim even came from?, was it from some study? I know the help screen/manual includes info from some study (from memory, brain fade here) that only 60% of central apnea has an open airway present, the other 40% may be closed.rested gal wrote:That's what I'm questioning..that 100% accuracy of the 420E in being correct - always correct - when it says "Now, THAT's a central apnea." I always thought the 420E would be right about that. Now I wonder.Snoredog wrote:My understanding is the 420e only scores CA's on line 2 when it hears cardiac oscillations associated with an open airway. So for the CA's found on line 2, it hears cardiac oscillations associated and is 100% accurate in those detections.
At the same time the 420E was chalking up those centrals for me, the PSG equipment was saying "centrals = zero."
SAG's interpretation above of the 420's ability to detect cardiac oscillations over a closed air way is new to me. I thought it was looking for those associated with a inhale. Is cardiac pulsation the same thing? (I'm no cardiologist).
So if your airway is closed and you are experiencing a central apnea, are you not having an obstructive apnea at that point? If you were manually scoring these, where would you report the central event with the closed airway? Let's see, the airway is blocked, there is no airflow, that is a obstructive apnea to me.
For examples sake, lets say machine detects 10 central apnea. Based on that help screen study, 6 of those 10 (avg) would have an associated "open" airway, if the airway is open the machine can hear/sense the cardiac oscillations and see absence of airflow.
So it is looking at 2 parameters in determining if the event is central, then if it is to respond, additional parameters such as current delivery pressure, command on apnea value. That by itself makes the 420e much more accurate then the latest auto's on the market which only look at absence of airflow and the latter parameters.
So if we assume that 6 of those 10 had open airways with cardiac oscillations, then they would be scored on line 2 as "Apnea/CA". The other 4 centrals would be scored under line 1 as simply Apnea (obstructive).
So if the 420e scored those 4 centrals (with the closed airway) as "obstructive" on line 1, then it would be technically incorrect when scoring those 4 events or would it?
So based upon the 420e's own admission, the 420e is 60% accurate in scoring central apnea, BUT of those it scored on line 2 it would be 100% accurate based upon its own selection criteria. By simply looking at the additional parameter of cardiac oscillations, the 420e is obviously more accurate in differentiating the event than nearly all other cpap autos on the market.
I wonder what the real difference is with the AdaptSV type machines, are they simply doing a better job with differentiating central apnea from obstructive? Are they also listening for cardiac oscillations like the 420e has been doing for years?
The sensor contained in the Remstar for example has always been able to detect cardiac oscillations just like the 420e but for unknown reasons they never implemented it within the firmware/software, the ability to do so has always been there. I know the S7 Spirit wasn't capable of doing that, the S8 now is, but they didn't implement it either. Maybe PB has the patent on that, I don't know.
Lab PSG accuracy: You have more experience with that than I on that front, but my understanding is those are "manually" scored and subject to the interpretation of the tech doing the scoring observing and interpreting the event on the EEG. Is the lab's transducers any more accurate/sensitive than the ones used inside the machine? I don't know, I know Dr. Sullivan has questioned the accuracy/sensitivity of the lab transducer in the past.
We pulled up the Honeywell (think it was the 9000 series) transducer/Phenumotach sensor once, if I recall correctly the device is pretty accurate and sensitive enough to actually sense CO2 levels. After seeing that I brought up the question why they didn't take advantage of that function/feature in the design of the AdaptSV machines, seems to me if you are going to pay so much attention to dead space and mask exhaust rates that the machine could detect changing CO2 levels. But I guess while the device may be capable of actually doing that, getting it do do that accurately from the end of a 2m hose is a bit of a challenge.
Notice that the 420e has the smaller pressure sensor line right at the mask, then some of the Resmed SV style machines have the same, are they measuring pressure (sure they are) or are they also measuring CO2 levels, who knows.
When you think about it, finger pulse oximeter is not very accurate either.
I know we have seen many patients show up here with Zero CA's listed on their PSG reports then they have another titration with another tech and they magically appear (are they like me I didn't have any night before last). How do we know?
I know with my own case, I don't have them every night and other nights I may have a dozen (making no changes to the machine). Last night I had 2 at what appear to be about the time I was in REM and yet the night before I had zero and I woke up at 4AM wide awake and couldn't get back to sleep, reason I looked at the report, I didn't have any obstructive apnea, no centrals only about 6 or so hypopnea. Last night when I had the 2 CA's logged, I actually felt better today.
I sold my house and in the process of moving near Sacramento, so i've been doing alot of work packing so I've been pretty dead by the time night comes around.
After seeing numerous Remstar reports and LCD data, I have a much higher confidence level with the 420e being accurate with its data than say the Remstars. I think the Encore reports are much more accurate than the LCD and there can be many reasons for that.
I mean when you look at it, Silverling software has been out what 6 or 7 years now? with not many changes that I can tell, about all I've seen from 3.0 was them adding the additional machines to the library when they came out with the 420 series and later the 425 series. 3.0 worked as well as 3.2, if they came out with 3.3 don't think i would buy it.
someday science will catch up to what I'm saying...
That makes sense to me - the detailed record presentation is a "60 second sampling condensed display of signals and events detected" (according to the manual, Revision E page 32). So any events occuring within one minute will look simultaneous, even if they aren't.Snoredog wrote:is there normally a pause between say an obstructive apnea and a post-arousal central?StillAnotherGuest wrote: On the other hand, trying to explain that simultaneous obstructive apnea/central apnea/hypopnea might be a little difficult.
For example; patient starts off with a hypopnea (10 sec, >50% flow), develops into a full apnea (>10sec, 0% flow) then is followed by a post-arousal central,
would that not produce the vertically aligned events you zoomed in on above?
I really don't know the duration of a "tic" on a 420e or time it represents, I would assume it is 10 seconds?
Since...
Flow limitation is reduction in air flow of <50% flow lasting 10 seconds or longer,
Hypopnea is reduction in flow of >50% lasting 10 seconds or longer in duration
Apnea is occluded or no flow.
My understanding is the 420e only scores CA's on line 2 when it hears cardiac oscillations associated with an open airway. So for the CA's found on line 2, it hears cardiac oscillations associated and is 100% accurate in those detections.
Its only the real time recording the shows every 10 seconds.
Me too.rested gal wrote:That's what I'm questioning..that 100% accuracy of the 420E in being correct - always correct - when it says "Now, THAT's a central apnea." I always thought the 420E would be right about that. Now I wonder.
Cardiogenic Oscillations on the Airflow Signal During Continuous Positive Airway Pressure as a Marker of Central Apnea* This is from 1999.
Methods: We examined 648 apneas in 52 patients undergoing nocturnal polysomnograms and CPAP titrations. Airflow was measured using the output of the CPAP generator, and apneas were identified from reduction of airflow to < 10% for > 10 s. We used only the presence or complete absence of thoracoabdominal motion to classify apneas: obstructive apnea when motion was present (297 apneas); and central apnea if motion was totally absent (351 apneas). Central apneas most often occurred at sleep onset or followed arousal with a big breath. Using only the flow signal, all apneas were examined for the presence of cardiogenic oscillation by an observer blinded to other signals and apnea types.
Results: No obstructive apnea showed definite cardiogenic oscillations. In four cases, there was a suggestion of oscillation that was not regular enough to be called cardiac. Sixty percent of central apneas showed clear, regular oscillations at cardiac frequency. Cardiogenic oscillations also were seen intermittently during quiet exhalation in apnea-free periods.
I'm emphasising the results:
1. No obstructive apnea showed definite cardiogenic oscillations. (if it has definite cardiac oscillations, its not obstructive)
2. In four cases, (out of 648 apneas?) there was a suggestion of oscillation that was not regular enough to be called cardiac. (a human scorer would know the difference)
3. (Only) Sixty percent of central apneas showed clear, regular oscillations at cardiac frequency.
4. Cardiogenic oscillations also were seen intermittently during quiet exhalation in apnea-free periods
So -- does the SL3 reporting module for the 420e distinguish between 3 and 4? In other words, does the SL3 reporting module, while reading the 420E data. record "apnea c/a" only in the presence of cardiogenic oscillations with concurrent/b] airflow cessation?
Not according to rested gal's data.
O.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
-
rested gal
- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
I don't know what study it was from either. Here's what -SWS quoted from, I think, a 418 manual:Snoredog wrote:to be honest, I really don't know where that "100% accuracy" claim even came from?, was it from some study? I know the help screen/manual includes info from some study (from memory, brain fade here) that only 60% of central apnea has an open airway present, the other 40% may be closed.
viewtopic.php?t=754
As I understand it:
62% sensitivity means...38% of centrals will go by unnoticed by the 420E. It will notice 62% of them, but will miss seeing a lot of them.
Of the 62% centrals it does notice, it will be correct 100% of the time in calling those "centrals."
But...there's that PSG night....
I still think the sensor tube in the 420E's air hose was inadvertently kinked or pinched or somethin'. That number of centrals hasn't shown up for me before or since.
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
I think you are right, I also thought we had a similar discussion on this topic before then (on another board) years ago along the same lines with Ted, Perry & SWS.rested gal wrote:I don't know what study it was from either. Here's what -SWS quoted from, I think, a 418 manual:Snoredog wrote:to be honest, I really don't know where that "100% accuracy" claim even came from?, was it from some study? I know the help screen/manual includes info from some study (from memory, brain fade here) that only 60% of central apnea has an open airway present, the other 40% may be closed.
viewtopic.php?t=754
someday science will catch up to what I'm saying...
Lets put it differenly: what was it about your machine that had it picking up cardiac oscillation, without picking up the accompanying "quiet exhalations" that seem to have been picked up in PSG ?rested gal wrote:I don't know what study it was from either. Here's what -SWS quoted from, I think, a 418 manual:Snoredog wrote:to be honest, I really don't know where that "100% accuracy" claim even came from?, was it from some study? I know the help screen/manual includes info from some study (from memory, brain fade here) that only 60% of central apnea has an open airway present, the other 40% may be closed.
viewtopic.php?t=754
As I understand it:
62% sensitivity means...38% of centrals will go by unnoticed by the 420E. It will notice 62% of them, but will miss seeing a lot of them.
Of the 62% centrals it does notice, it will be correct 100% of the time in calling those "centrals."
But...there's that PSG night....
I still think the sensor tube in the 420E's air hose was inadvertently kinked or pinched or somethin'. That number of centrals hasn't shown up for me before or since.
Oh. What was you IFL1 and 2 set on for that night?
O.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): 420E, hose
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
-
rested gal
- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
IFL1 was off, and IFL2 was on -- both set as usual.ozij wrote:Oh. What was you IFL1 and 2 set on for that night?
O.
Main air hose hung overhead, as usual.
Decapitated "Headrest" mask, as usual.
Mouth taped, as usual.
PAPillow used, as usual.
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
-SWS was looking at product decription , (that didn't have 100% in it), and referred to "independent studies" in general.
Based on the paper I quoted, and on what we see, I'm beginning to think that 100% is something we may have made up along the way.
The PB may be 100% reliable in not responding to when it here's cardiac oscillations you can trust it to do that (so chances of increased pressure for central apneas are better), but it isn't necessarily 100% right in reporting the existence of central apneas. Its not a good diagnostic device.
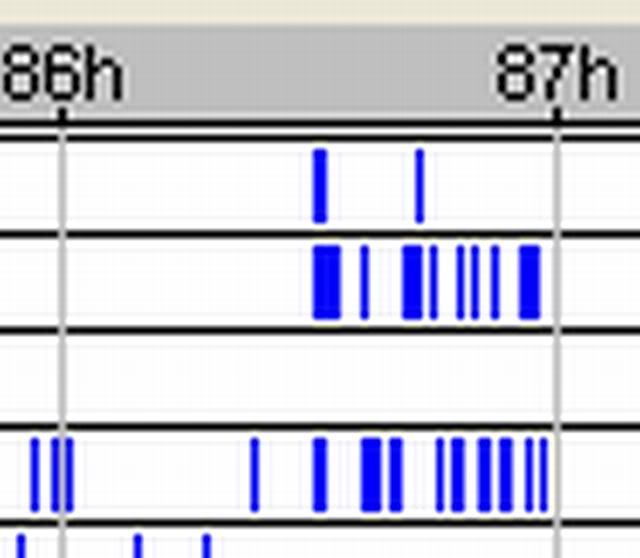
If you look at your data, rested gal, you'll see practically all your apnea with cardiac oscillation come with hypopneas.
Maybe it's ticking off those cardiac oscillations because it picks them up while you doing "quite inalation and exhalation" that it is misintepreting as hypopneas (due to a kink in the tube?)?
I keep thinking of the way they droppend both "mixed" and "central" apneas as descriptive terms in the 420e manual - after having used them for the 418p. Maybe they figured the data wasn't reliable enough for calling them that.
And the 418p detailed record was a 30 second sampling, while the 420e's is a 60 second sampling - which also makes it less accurate.
O.
O.
Based on the paper I quoted, and on what we see, I'm beginning to think that 100% is something we may have made up along the way.
The PB may be 100% reliable in not responding to when it here's cardiac oscillations you can trust it to do that (so chances of increased pressure for central apneas are better), but it isn't necessarily 100% right in reporting the existence of central apneas. Its not a good diagnostic device.
If you look at your data, rested gal, you'll see practically all your apnea with cardiac oscillation come with hypopneas.
Maybe it's ticking off those cardiac oscillations because it picks them up while you doing "quite inalation and exhalation" that it is misintepreting as hypopneas (due to a kink in the tube?)?
I keep thinking of the way they droppend both "mixed" and "central" apneas as descriptive terms in the 420e manual - after having used them for the 418p. Maybe they figured the data wasn't reliable enough for calling them that.
And the 418p detailed record was a 30 second sampling, while the 420e's is a 60 second sampling - which also makes it less accurate.
O.
O.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
I found this white paper from 2004 doing a clinical evaluation of the PB420E.
http://www.puritanbennett.com/_Catalog/ ... 0Paper.pdf
You can't copy and paste from it,... but at least the did try to compare the 420e ability to detect events to a psg's.
It's at its worst when dealing with "non apneic respiratory events" (Hypopneas and episodes or RUNs of flow limitations).
PSG data was divided into 1 minute epochs to assess concordance between the device's events detecting and the PSG's respiratory scoring.
An interesting read.
O.
http://www.puritanbennett.com/_Catalog/ ... 0Paper.pdf
You can't copy and paste from it,... but at least the did try to compare the 420e ability to detect events to a psg's.
It's at its worst when dealing with "non apneic respiratory events" (Hypopneas and episodes or RUNs of flow limitations).
PSG data was divided into 1 minute epochs to assess concordance between the device's events detecting and the PSG's respiratory scoring.
An interesting read.
O.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023