






carla,
since i know you:) i can tell you that i think both snoredog and rested_gal are spot on. i think there are variable factors influencing your treatment....
the GERD possibility fits with some of your hx to which i'm privvy and fits in just right with the whole allergy/asthma thing.
all of those tricky bits coming together to cause problems with the rx'ed course of action.
the provigil isn't going to be an option if you're planning on a pregnancy soon. it's going to be cpap (or apap or whatever) and maybe at most nasal steroids.
hopfully soon you'll get this mask thing straightened around so that you're clear enough to deal with other interventions that might be helpful - dietary, enzymes, minerals. krispin might have some helpful suggestions or the possible plm issue. i'd suspect it's going to involve sufficient minerals and hmmm, sufficient vitamin D.....and sufficient potassium. Imagine that.
k
Help! Still Sleepy, MyEncore Reports, etc.
-
Guest
Carla: You may also want to compare your 12/4-12/5 data at the bottom, you will see you ran all the way up to 19cm pressure!! Again you were titrated at 13 but you start having central events at 10.6cm pressure. You will see in the data that the NR events begin at 11cm pressure and only get worse from there.
Note: some of those centrals I highlighted on the OA line are probably a mix of central and mixed events vs all being central.
Snore data: you should also compare your 12/4's snore data to the next night on 12/6, you will see much fewer snores, you also see better results. 12/6 fewer snores better cpap results however your pressure still ran up to 17cm which I see as being a problem. A glass of wine with dinner can make a person snore much more one night vs the other, taking a allergy medication could have the same result.
Large Leak on 12/6: When ever you see that black solid line at the top of the Leak chart, that means the machine CANNOT respond to OSA events, in fact the Remstar won't respond to events when that is detected.
You have a severe problem with leaks, the leak can even be internal like from the humidifier tank gasket, make sure the tank is seated properly. There is also a gasket where the machine connects to the humidifier platform, you might want to check it, you check it by removing the humidifier tank, close the barn door, put your left hand on the humidifier to hold it down, then grasp the lip on the front of the machine about 1/2" up from the bottom and lift up on the machine firmly. This will separate the machine from the humidifier platform, if the gasket looks okay reinstall in reverse order. If there are no leaks from the machine or the hose then you have a problem with the Hybrid, 75L/m is way too much but that can also be from the runaway pressure you are experiencing.
Note: some of those centrals I highlighted on the OA line are probably a mix of central and mixed events vs all being central.
Snore data: you should also compare your 12/4's snore data to the next night on 12/6, you will see much fewer snores, you also see better results. 12/6 fewer snores better cpap results however your pressure still ran up to 17cm which I see as being a problem. A glass of wine with dinner can make a person snore much more one night vs the other, taking a allergy medication could have the same result.
Large Leak on 12/6: When ever you see that black solid line at the top of the Leak chart, that means the machine CANNOT respond to OSA events, in fact the Remstar won't respond to events when that is detected.
You have a severe problem with leaks, the leak can even be internal like from the humidifier tank gasket, make sure the tank is seated properly. There is also a gasket where the machine connects to the humidifier platform, you might want to check it, you check it by removing the humidifier tank, close the barn door, put your left hand on the humidifier to hold it down, then grasp the lip on the front of the machine about 1/2" up from the bottom and lift up on the machine firmly. This will separate the machine from the humidifier platform, if the gasket looks okay reinstall in reverse order. If there are no leaks from the machine or the hose then you have a problem with the Hybrid, 75L/m is way too much but that can also be from the runaway pressure you are experiencing.
-
curtcurt46

- Posts: 262
- Joined: Wed Sep 27, 2006 12:35 pm
- Location: Retired US Army
Carla,
I believe rested gal may be on to something. Your bad nights may be related to upper respiratory congestion and GERD. Either one of them can have an impact on your airway. If they are both in play then you are getting a double wammy.
I know, I have allergies that cause congestion and I also my have GERD, but this has not be confirmed by an ENT.
Here is what happened to me two days ago. This same situation may apply to you.
I didn't take my antihistamine for the whole day. I wanted to reduce the stuff I take. Sure enough I had an AHI of 5.4 along with 1 NR apnea. My running avg is around 1.2 AHI. At this point I didn't realize what was going on. Last night I had an 8.6 AHI and was even more congested when I woke in the morning. It was then, that I realized the my chest was not clear and I had not taken the antihistamines. I also took an expectorant (Mucinex) to clear out the UR. Also, an interesting fact was that my variable breathing hit 42% and 55% respectively. On a normal night my VB is 15% - 18%. I get this data from My Encore. Variable breathing is defined as the situation when a person is not undergoing the quiet steady breathing of several stages of sleep. Variable breathing happens during wakefulness, distress, and REM. It's the distress part I am experiencing and you may be experiencing.
You might look at My Encore and look at the VB and see if your % isn't high on the nights with high AHI's. I bet your VB for the Dec 7th was lower and more to a normal.
I also looked at your charts and I don't see centrals despite some other theories. The Encore Pro software is not capable of detecting a central apnea and the only way to know for sure is to go to the sleep lab and get hooked up to all the channels.
Let us know how your therapy improves.
I believe rested gal may be on to something. Your bad nights may be related to upper respiratory congestion and GERD. Either one of them can have an impact on your airway. If they are both in play then you are getting a double wammy.
I know, I have allergies that cause congestion and I also my have GERD, but this has not be confirmed by an ENT.
Here is what happened to me two days ago. This same situation may apply to you.
I didn't take my antihistamine for the whole day. I wanted to reduce the stuff I take. Sure enough I had an AHI of 5.4 along with 1 NR apnea. My running avg is around 1.2 AHI. At this point I didn't realize what was going on. Last night I had an 8.6 AHI and was even more congested when I woke in the morning. It was then, that I realized the my chest was not clear and I had not taken the antihistamines. I also took an expectorant (Mucinex) to clear out the UR. Also, an interesting fact was that my variable breathing hit 42% and 55% respectively. On a normal night my VB is 15% - 18%. I get this data from My Encore. Variable breathing is defined as the situation when a person is not undergoing the quiet steady breathing of several stages of sleep. Variable breathing happens during wakefulness, distress, and REM. It's the distress part I am experiencing and you may be experiencing.
You might look at My Encore and look at the VB and see if your % isn't high on the nights with high AHI's. I bet your VB for the Dec 7th was lower and more to a normal.
I also looked at your charts and I don't see centrals despite some other theories. The Encore Pro software is not capable of detecting a central apnea and the only way to know for sure is to go to the sleep lab and get hooked up to all the channels.
Let us know how your therapy improves.
Curtis
curtcurt46
curtcurt46

RG:rested gal wrote:Carla, thank you for putting the PDF of several nights of "Daily Details" from your Encore Pro report up on your website.
I'm not a doctor. Just guessing. I would strongly suspect GERD as the culprit interfering with smooth treatment from your autopap.
It was most interesting that the last "detailed" night (Dec 7 -8) showed a night of very smooth treatment and low AHI. If GERD is a problem for you, I'd think that was a night of not much acid reflux activity. And I'd wonder if the other nights were when GERD was acting up badly. Even if you have never noticed any signs of "heartburn", there's such a thing as "Silent GERD" with no symptoms that you'd notice. Can really wreck cpap treatment.
I'd look very, very seriously into untreated and/or undertreated GERD (gastroesophageal reflux disease.) If that is the problem, it isn't going to matter what mask you use, what machine, what settings. Positive Air Pressure is not able to push aside swollen, rigid tissues or spasming vocal cords. GERD (if that's an underlying problem) would have to be treated first.
Like I said, I'm not a doctor. Just my two cents.
Check out these topics:
Nov 05, 2005 subject: SUCCESS AT LAST-GERD,420E, PRILOSEC AND BENADRYL -SWS's thoughts on loonlvr's massive clusters of events and loonlvr's followup post.
viewtopic.php?t=5551
Oct 09, 2006 subject: My Sinus problem cure Kazoo's allergist doctor spots continued acid reflux problems despite Kazoo being on the "Purple Pill" (Nexium)
viewtopic.php?t=14189
Apr 28, 2006 subject: Articles about Acid Reflux, Sinus and Nasal congestion. Links posted by RestInSeattle
viewtopic.php?p=95185
Do you know of any scientific links explaining the etiology behind this Silent GERD and Obstructive Sleep Apnea connection?
I understand one can exist with the other but I have yet to read where reflux can contribute to more SDB events and/or resemble central events. I can see where if the vocal cords are continually saturated with stomach acid from the reflux there could be dysfunction there.
But in all the searches I've done about all I can find is that GI press release from Duke University at the 70th Annual Scientific Meeting of the American College of Gastroenterology. It reads more like another group of doctors wanting to cash in on their piece of the proverbial OSA money pie:
http://www.news-medical.net/?id=14207
http://www.sciencedaily.com/releases/20 ... 080008.htm
http://www.chestjournal.org/cgi/reprint/124/2/767.pdf
http://www.sleepapneainfo.com/cov.php?page=10
http://www.endonurse.com/articles/5c1briefs.html
Man reading all these is like watching Tom Cruise appear in the morning on the Today Show, then Oprah, then Conan, then Last Call with Carson Daily. I sure wish Jerry Springer would come to NBC
Maybe I'm looking in the wrong place but I cannot find anything that would substantiate the link. We know if you are laying down and gasp for air after a SDB event it can create a vacuum in the esophagus with such force it can suck up stomach acid all the way up to the mouth. It is even thought to be one of the leading causes of Periodontal disease .
Sorry but I don't buy the GERD link especially in Carla's case, if you compare the last Auto-Daily report on 12/7-12/8 where she was only at 9cm pressure it resulted in the lowest AHI of 2.1. That daily report shows leaks under control, all events being addressed and she never went above 10cm pressure. If lower pressure results in better sleep why not limit one to lower pressure. If she sets her maximum pressure to 10cm as suggested she should have many more nights like that shown on the 12/7-12/8 report.
-
curtcurt46
- Posts: 262
- Joined: Wed Sep 27, 2006 12:35 pm
- Location: Retired US Army
Snoredog,
Here are three articles that link GERD with SDB.
http://medicalnewstoday.com/medicalnews ... wsid=13671
http://medscape.com/viewarticle/516189
You have to register, but it's free.
http://www.grandtimes.com/GERD.html
I would ask you how you determined that Carla was having pressure induced events.
Certainly MyEncore and Encore Pro can't tell you that. The fact is only a full blown PSG can tell you this.
I think you are looking at the reports and making conclusions that are not supported in fact.
The apap records the events as they occur. The fact that at a particular pressure a number of events occurred does not indicate the the apap caused the event. It does indicate that the event was resolved at that pressure. Why the pressure had to go that high goes back to the various controllers and algorithms at play.
Have you looked at her variable breathing on the nights of higher AHI's?
The VB indicates a situation of wakefulness, REM or distresss. It's the distress that is causing the higher AHI numbers. Her distress based on her own admission may well be upper respiratory congestion from allergies and asthma. This in fact can play a big role in the ability of apap to deliver the correct and best therapy. GERD may also be at play, but we simply don't know at this point for sure.
The truth is that neither of us knows for sure. Only Carla along with good medical care can determine the the factors that effect her therapy.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): Encore Pro, AHI, APAP
Here are three articles that link GERD with SDB.
http://medicalnewstoday.com/medicalnews ... wsid=13671
http://medscape.com/viewarticle/516189
You have to register, but it's free.
http://www.grandtimes.com/GERD.html
I would ask you how you determined that Carla was having pressure induced events.
Certainly MyEncore and Encore Pro can't tell you that. The fact is only a full blown PSG can tell you this.
I think you are looking at the reports and making conclusions that are not supported in fact.
The apap records the events as they occur. The fact that at a particular pressure a number of events occurred does not indicate the the apap caused the event. It does indicate that the event was resolved at that pressure. Why the pressure had to go that high goes back to the various controllers and algorithms at play.
Have you looked at her variable breathing on the nights of higher AHI's?
The VB indicates a situation of wakefulness, REM or distresss. It's the distress that is causing the higher AHI numbers. Her distress based on her own admission may well be upper respiratory congestion from allergies and asthma. This in fact can play a big role in the ability of apap to deliver the correct and best therapy. GERD may also be at play, but we simply don't know at this point for sure.
The truth is that neither of us knows for sure. Only Carla along with good medical care can determine the the factors that effect her therapy.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): Encore Pro, AHI, APAP
Curtis
curtcurt46
curtcurt46
No no, I already acknowledged that OSA and GERD are commonly found together, I'm not questioning that, pretty much anyone that has OSA already knows that. You can list 50 links to news and journal articles and I already know that, that is not what I am questioning.curtcurt46 wrote:Snoredog,
Here are three articles that link GERD with SDB.
http://medicalnewstoday.com/medicalnews ... wsid=13671
http://medscape.com/viewarticle/516189
You have to register, but it's free.
http://www.grandtimes.com/GERD.html
I would ask you how you determined that Carla was having pressure induced events.
Certainly MyEncore and Encore Pro can't tell you that. The fact is only a full blown PSG can tell you this.
I think you are looking at the reports and making conclusions that are not supported in fact.
The apap records the events as they occur. The fact that at a particular pressure a number of events occurred does not indicate the the apap caused the event. It does indicate that the event was resolved at that pressure. Why the pressure had to go that high goes back to the various controllers and algorithms at play.
Have you looked at her variable breathing on the nights of higher AHI's?
The VB indicates a situation of wakefulness, REM or distresss. It's the distress that is causing the higher AHI numbers. Her distress based on her own admission may well be upper respiratory congestion from allergies and asthma. This in fact can play a big role in the ability of apap to deliver the correct and best therapy. GERD may also be at play, but we simply don't know at this point for sure.
The truth is that neither of us knows for sure. Only Carla along with good medical care can determine the the factors that effect her therapy.
I'm questioning where having GERD or silent GERD or Laryngopharyngeal reflux, or LPR is shown to increase the frequency of SDB events to the scale shown on Carla's reports from one night to the other and how those events can show up as NR to the machine.
I'd like to KNOW what factors say it is GERD or LPR or Centrals as in Carla's case? I know the latter, I have the disorder myself.
You also jumped on the GERD bandwagon as the conclusion in Carla's case so you must also know, so if you don't mind please explain to us how this condition can increase the frequency of SDB events seen?
My suggestion is easy, all she has to do is try the new settings and pull a report the next day. What can she do with GERD or LPR to see results the next day? Sleep standing up?
I'm using her data to make my decision, I'm not just throwing a dart.
-
curtcurt46
- Posts: 262
- Joined: Wed Sep 27, 2006 12:35 pm
- Location: Retired US Army
Snoredog wrote:
"No no, I already acknowledged that OSA and GERD are commonly found together, I'm not questioning that, pretty much anyone that has OSA already knows that. You can list 50 links to news and journal articles and I already know that, that is not what I am questioning.
I'm questioning where having GERD or silent GERD or Laryngopharyngeal reflux, or LPR is shown to increase the frequency of SDB events to the scale shown on Carla's reports from one night to the other and how those events can show up as NR to the machine.
I'd like to KNOW what factors say it is GERD or LPR or Centrals as in Carla's case? I know the latter, I have the disorder myself.
You also jumped on the GERD bandwagon as the conclusion in Carla's case so you must also know, so if you don't mind please explain to us how this condition can increase the frequency of SDB events seen?
My suggestion is easy, all she has to do is try the new settings and pull a report the next day. What can she do with GERD or LPR to see results the next day? Sleep standing up?
I'm using her data to make my decision, I'm not just throwing a dart."
I believe you are the one throwing the dart.
Did you read the articles? They lead me to believe that GERD can have an impact on breathing and in turn influence the events that occur. I concluded by saying the GERD might be at play but simply don't know for sure.
I really focused on the distress that might be caused by an upper respiratory condition. Did you look at her VB? Her numbers are high on her worse nights. I would have to read the apap patent to better understand what the machine does during VB, but its my guess the machine is limited during this type event because of the lack of being able to predict a solution.
Also, you did not address the underlying issue as to whether in Carla's case the machine is causing pressure induce events or it is responding to flow and the events are resloved at a particular pressure.
If Carla addresses the upper respiratory situation, with or without GERD, satisfactorly then she will see improvements in her stats. This is provided she addresses the leaks and a correct pressure is established.
I close by saying that Carla along with good medical care can find the causes that effect her therapy and in turn make the necessary adjustments to give her the best therapy possible.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): news, APAP
"No no, I already acknowledged that OSA and GERD are commonly found together, I'm not questioning that, pretty much anyone that has OSA already knows that. You can list 50 links to news and journal articles and I already know that, that is not what I am questioning.
I'm questioning where having GERD or silent GERD or Laryngopharyngeal reflux, or LPR is shown to increase the frequency of SDB events to the scale shown on Carla's reports from one night to the other and how those events can show up as NR to the machine.
I'd like to KNOW what factors say it is GERD or LPR or Centrals as in Carla's case? I know the latter, I have the disorder myself.
You also jumped on the GERD bandwagon as the conclusion in Carla's case so you must also know, so if you don't mind please explain to us how this condition can increase the frequency of SDB events seen?
My suggestion is easy, all she has to do is try the new settings and pull a report the next day. What can she do with GERD or LPR to see results the next day? Sleep standing up?
I'm using her data to make my decision, I'm not just throwing a dart."
I believe you are the one throwing the dart.
Did you read the articles? They lead me to believe that GERD can have an impact on breathing and in turn influence the events that occur. I concluded by saying the GERD might be at play but simply don't know for sure.
I really focused on the distress that might be caused by an upper respiratory condition. Did you look at her VB? Her numbers are high on her worse nights. I would have to read the apap patent to better understand what the machine does during VB, but its my guess the machine is limited during this type event because of the lack of being able to predict a solution.
Also, you did not address the underlying issue as to whether in Carla's case the machine is causing pressure induce events or it is responding to flow and the events are resloved at a particular pressure.
If Carla addresses the upper respiratory situation, with or without GERD, satisfactorly then she will see improvements in her stats. This is provided she addresses the leaks and a correct pressure is established.
I close by saying that Carla along with good medical care can find the causes that effect her therapy and in turn make the necessary adjustments to give her the best therapy possible.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): news, APAP
Curtis
curtcurt46
curtcurt46
curtcurt46 wrote:
This is a Remstar Auto it doesn't record variable breathing (VB), maybe if it was a AutoBipap it would, but not the Auto. Don't confuse variable breathing with erratic breathing after an event.
I'm looking at her last 4-day EncorePro report, go to the very last page under Remstar Auto Statistics, it says Auto-CPAP Mean Pressure = 10.6cm then it says Auto-CPAP "Peak" Average Pressure=17cm. Mean is the average pressure over the 4 day period (forget the highs and lows), then Peak is the average Peak seen over same 4-day period. If you look at the individual days compare the events with pressure used, her data looks good on all days when she stays under 10cm, the higher pressure goes the more events are seen.
Not too hard to see,
12/5 - 90% pressure was 15cm, AHI=15.1
12/6 - 90% pressure was 17cm, AHI=4.0
12/7 - 90% pressure was 14cm, AHI=8.7
12/8 - 90% pressure was 9cm, AHI=2.4 best of the 4-day period, also lowest 90% pressure.
Look at the last 12/8 daily report, leaks are well under control, pressure didn't go to high OA is not bad at 1.7, HI=0.8. She still had an average leak rate of 53.71L/m which is a bit high but that is due to use of the Hybrid mask, its exhaust leaks like a sieve.
The problem you need to understand with the reports is the machine reports central apnea as obstructive, this skews the data you are looking at. Large leak also skews the data, but that goes hand in hand with higher pressure. The ONLY time the machine "discards" the OA data is when it effectively logs an NR event (it tosses out the previous triple event). Now if there were only 2 apnea events not correctly scored, those 2 apneas go into the machines sample data stored in memory as obstructive so when it sees them again it may increase pressure making them actually worse. That is why the number of events increase with pressure.
If those events were obstructive apnea (even if caused by GERD in your therory) then pressure should stent them where the frequency reduces, but that is NOT the case here they increase in frequency as the pressure increases.
If the machine is not scoring apnea correctly you then have to question those hypopnea and even Flow limitations as well as they are even harder to distinguish.
How many of those Hypopnea reported are possibly central hypopnea vs obstructive hypopnea?
Nearly impossible to detect accurately without EEG and respiratory straps as used in a PSG.
If the Remstar is logging ANY NR events you can pretty much be assured it is not scoring other events accurately either. But that is not all bad you can still use the data to your advantage, if you know you are at risk of that disorder and that is what the NR flags are for to tell you there is a problem. Then you can do simple things to limit the exposure to them. You don't get any awards for using higher pressure.
If she keeps her maximum pressure under 10.cm leaks will become better controlled, she will have fewer events, data seen will be more accurate, her aerophagia will get better. It is shown in every report she has put up.
If you guys are suggesting she has worse nights compared to others because of GERD that doesn't really matter.
It is what the machine is doing when she does have those worse nights whatever the reason may be.
Set the machine to the parameters I suggested and her worst night will be no worse than the 12/8's data shown even if she eats spaghetti for dinner.
On those worst nights her machine may peg or flat-line at 10cm, that is no big deal, the events causing the machine to want to go higher are being misread anyway. The increase from 5cm to 6cm on the Min pressure would probably reduce the FL's if that is what they truly are.
Don't think so bud, where are you getting this variable breathing data?I believe you are the one throwing the dart.
Did you read the articles? They lead me to believe that GERD can have an impact on breathing and in turn influence the events that occur. I concluded by saying the GERD might be at play but simply don't know for sure.
I really focused on the distress that might be caused by an upper respiratory condition. Did you look at her VB? Her numbers are high on her worse nights. I would have to read the apap patent to better understand what the machine does during VB, but its my guess the machine is limited during this type event because of the lack of being able to predict a solution.
Also, you did not address the underlying issue as to whether in Carla's case the machine is causing pressure induce events or it is responding to flow and the events are resolved at a particular pressure.
If Carla addresses the upper respiratory situation, with or without GERD, satisfactorly then she will see improvements in her stats. This is provided she addresses the leaks and a correct pressure is established.
I close by saying that Carla along with good medical care can find the causes that effect her therapy and in turn make the necessary adjustments to give her the best therapy possible.
This is a Remstar Auto it doesn't record variable breathing (VB), maybe if it was a AutoBipap it would, but not the Auto. Don't confuse variable breathing with erratic breathing after an event.
I'm looking at her last 4-day EncorePro report, go to the very last page under Remstar Auto Statistics, it says Auto-CPAP Mean Pressure = 10.6cm then it says Auto-CPAP "Peak" Average Pressure=17cm. Mean is the average pressure over the 4 day period (forget the highs and lows), then Peak is the average Peak seen over same 4-day period. If you look at the individual days compare the events with pressure used, her data looks good on all days when she stays under 10cm, the higher pressure goes the more events are seen.
Not too hard to see,
12/5 - 90% pressure was 15cm, AHI=15.1
12/6 - 90% pressure was 17cm, AHI=4.0
12/7 - 90% pressure was 14cm, AHI=8.7
12/8 - 90% pressure was 9cm, AHI=2.4 best of the 4-day period, also lowest 90% pressure.
Look at the last 12/8 daily report, leaks are well under control, pressure didn't go to high OA is not bad at 1.7, HI=0.8. She still had an average leak rate of 53.71L/m which is a bit high but that is due to use of the Hybrid mask, its exhaust leaks like a sieve.
The problem you need to understand with the reports is the machine reports central apnea as obstructive, this skews the data you are looking at. Large leak also skews the data, but that goes hand in hand with higher pressure. The ONLY time the machine "discards" the OA data is when it effectively logs an NR event (it tosses out the previous triple event). Now if there were only 2 apnea events not correctly scored, those 2 apneas go into the machines sample data stored in memory as obstructive so when it sees them again it may increase pressure making them actually worse. That is why the number of events increase with pressure.
If those events were obstructive apnea (even if caused by GERD in your therory) then pressure should stent them where the frequency reduces, but that is NOT the case here they increase in frequency as the pressure increases.
If the machine is not scoring apnea correctly you then have to question those hypopnea and even Flow limitations as well as they are even harder to distinguish.
How many of those Hypopnea reported are possibly central hypopnea vs obstructive hypopnea?
Nearly impossible to detect accurately without EEG and respiratory straps as used in a PSG.
If the Remstar is logging ANY NR events you can pretty much be assured it is not scoring other events accurately either. But that is not all bad you can still use the data to your advantage, if you know you are at risk of that disorder and that is what the NR flags are for to tell you there is a problem. Then you can do simple things to limit the exposure to them. You don't get any awards for using higher pressure.
If she keeps her maximum pressure under 10.cm leaks will become better controlled, she will have fewer events, data seen will be more accurate, her aerophagia will get better. It is shown in every report she has put up.
If you guys are suggesting she has worse nights compared to others because of GERD that doesn't really matter.
It is what the machine is doing when she does have those worse nights whatever the reason may be.
Set the machine to the parameters I suggested and her worst night will be no worse than the 12/8's data shown even if she eats spaghetti for dinner.
On those worst nights her machine may peg or flat-line at 10cm, that is no big deal, the events causing the machine to want to go higher are being misread anyway. The increase from 5cm to 6cm on the Min pressure would probably reduce the FL's if that is what they truly are.
I should add that if you read through these posts and understand what was said you will understand one of the main reason doctors are against autopap machines, is they can screw up even the best ones.
As RG suggested it may very well may be GERD or LPR as the underlying cause for the differences seen from one night to the next, but again it doesn't matter it is how the machine responds to those different conditions is what matters the most.
Under all circumstances you want to avoid central apnea especially pressure induced central apnea. Just like 32 second obstructive apnea, centrals are absent of air flow meaning no oxygen is getting to your lungs and vital organs, the heart responds the same by being overworked. They also interrupt your sleep more severely than other events even obstructive as they usually take you back to a fully wake state. You also feel like the walking dead the next day after having only a few.
If I was a sleep doctor instead of telling patients "No you cannot have a autopap" without any reason given, I'd drag out their PSG and show them why it is not suggested.
But even that doesn't mean you cannot use them, if you can learn to spot trends and setup up your machine accordingly you can easily use an autopap just as easy with all its added benefits and sleep more comfortably.
We should also not confuse the above condition with Cheyene-Stokes Respiration as that is a totally different disorder much more severe and associated with CHF.
Carla: if you try the suggested settings it would be interesting to see how you feel the next day and what your reports say.
As RG suggested it may very well may be GERD or LPR as the underlying cause for the differences seen from one night to the next, but again it doesn't matter it is how the machine responds to those different conditions is what matters the most.
Under all circumstances you want to avoid central apnea especially pressure induced central apnea. Just like 32 second obstructive apnea, centrals are absent of air flow meaning no oxygen is getting to your lungs and vital organs, the heart responds the same by being overworked. They also interrupt your sleep more severely than other events even obstructive as they usually take you back to a fully wake state. You also feel like the walking dead the next day after having only a few.
If I was a sleep doctor instead of telling patients "No you cannot have a autopap" without any reason given, I'd drag out their PSG and show them why it is not suggested.
But even that doesn't mean you cannot use them, if you can learn to spot trends and setup up your machine accordingly you can easily use an autopap just as easy with all its added benefits and sleep more comfortably.
We should also not confuse the above condition with Cheyene-Stokes Respiration as that is a totally different disorder much more severe and associated with CHF.
Carla: if you try the suggested settings it would be interesting to see how you feel the next day and what your reports say.
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
My guess is that good night was a night when she didn't have either GERD or congestion or allergies acting up and interfering with what any kind of PAP machine is designed to do... push aside soft tissue.Snoredog wrote:Sorry but I don't buy the GERD link especially in Carla's case, if you compare the last Auto-Daily report on 12/7-12/8 where she was only at 9cm pressure it resulted in the lowest AHI of 2.1.
Acid bathing the inside of the throat on a regular basis can cause irritation and swelling. Swollen tissue is more rigid. It's kinda' difficult for positive air pressure to push hard tissue aside to open the airway.
I'm not saying untreated or undertreated GERD causes OSA. I'm saying I think GERD making acid rise up into the airway can cause swollen tissue that makes it much more difficult for cpap/autopap/bipap/anypap to do it's job. The job being to splint open SOFT tissue.
I think if GERD's going on, all bets are off as to what pressure a person needs to use....'cause the situation doesn't really reflect what pressure (or range of pressures) are needed under "normal" circumstances..."normal" meaning just the "normal" OSA problem of SOFT tissues collapse or closure.
Please re-read this:
viewtopic.php?t=5551
-SWS once wrote: "Perhaps the biggest fallacy I have seen repeatedly mentioned on these message boards is that when a patient's AutoPAP cannot successfully treat their SDB [sleep disordered breathing] events, then at least their overnight data is going to be accurate. Nothing could really be further from the truth."
Again, I think perhaps that night reflected a night when Carla was not suffering from any number of underlying problems that can render cpap ineffective.Snoredog wrote:That daily report shows leaks under control, all events being addressed and she never went above 10cm pressure. If lower pressure results in better sleep why not limit one to lower pressure. If she sets her maximum pressure to 10cm as suggested she should have many more nights like that shown on the 12/7-12/8 report.
All the more reason, imho, to get those other things checked out thoroughly so a PAP machine is able to do what it can do so well -- splint soft tissue open.
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Okay I re-read it and can see where you made the link by comparing the apnea runs from loonlvr's to carla's, but did you also notice the 420E Silverlining is also reporting Apnea events as suspect as being CA shown on line2?rested gal wrote:My guess is that good night was a night when she didn't have either GERD or congestion or allergies acting up and interfering with what any kind of PAP machine is designed to do... push aside soft tissue.Snoredog wrote:Sorry but I don't buy the GERD link especially in Carla's case, if you compare the last Auto-Daily report on 12/7-12/8 where she was only at 9cm pressure it resulted in the lowest AHI of 2.1.
Acid bathing the inside of the throat on a regular basis can cause irritation and swelling. Swollen tissue is more rigid. It's kinda' difficult for positive air pressure to push hard tissue aside to open the airway.
I'm not saying untreated or undertreated GERD causes OSA. I'm saying I think GERD making acid rise up into the airway can cause swollen tissue that makes it much more difficult for cpap/autopap/bipap/anypap to do it's job. The job being to splint open SOFT tissue.
I think if GERD's going on, all bets are off as to what pressure a person needs to use....'cause the situation doesn't really reflect what pressure (or range of pressures) are needed under "normal" circumstances..."normal" meaning just the "normal" OSA problem of SOFT tissues collapse or closure.
Please re-read this:
viewtopic.php?t=5551
-SWS once wrote: "Perhaps the biggest fallacy I have seen repeatedly mentioned on these message boards is that when a patient's AutoPAP cannot successfully treat their SDB [sleep disordered breathing] events, then at least their overnight data is going to be accurate. Nothing could really be further from the truth."
Again, I think perhaps that night reflected a night when Carla was not suffering from any number of underlying problems that can render cpap ineffective.Snoredog wrote:That daily report shows leaks under control, all events being addressed and she never went above 10cm pressure. If lower pressure results in better sleep why not limit one to lower pressure. If she sets her maximum pressure to 10cm as suggested she should have many more nights like that shown on the 12/7-12/8 report.
All the more reason, imho, to get those other things checked out thoroughly so a PAP machine is able to do what it can do so well -- splint soft tissue open.
http://www.tnlc.com/Lara/laura/osa/loon ... nadryl.jpg
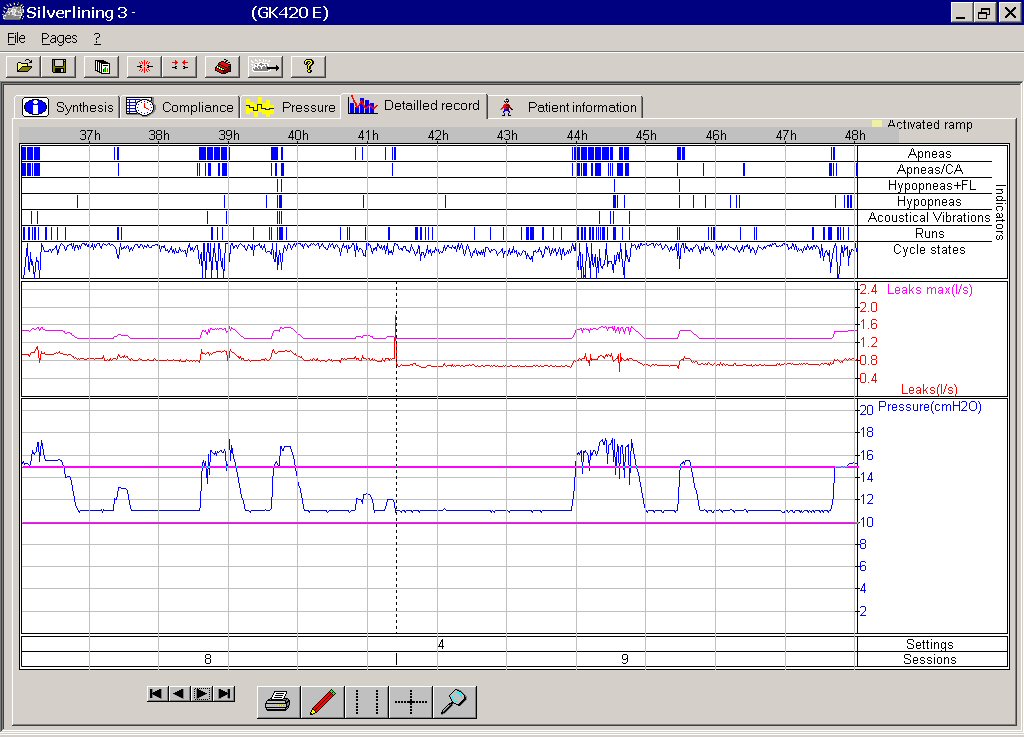{kind=link}
Interesting both machines are indicating CA events and the 420E is better equipped to detect them than the Remstar is (in my opinion).
And they do appear much better with after Prilosec:
http://www.tnlc.com/Lara/laura/osa/loon ... nadryl.jpg
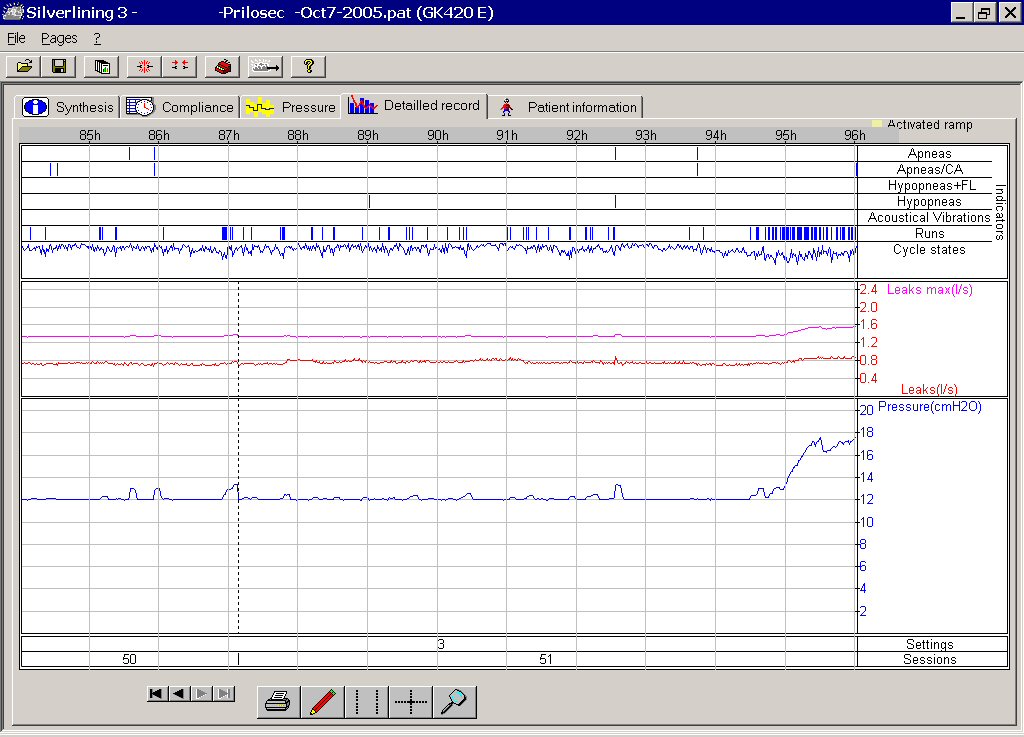{kind=link}
But can we positively conclude that Prilosec was what eliminated the central apnea? There is a huge difference between those. If so you may have come up with a cure for central apnea that Scientists have been struggling with for years.
Loonlvr's 2nd graph looks like Carla's 12/8 daily report, did she take Prilosec on that last night? There are no apnea runs or clusters shown on the 12/8 report like there is on previous night or on loonlvr's.
While we don't even know if she has GERD but we can assume so since we know it goes nearly hand in hand with OSA so that would not be unusual if she does (here we are giving her additional disorders hehehe).
The reason I wasn't buying into GERD aspect was I took prescription PrevAcid for a year which is much stronger than Prilosec you can buy, in fact my GP said he couldn't prescribe it to me and referred me to a GI Specialist where I had to first undergo general anesthesia for the endoscopy exam in the hospital as a outpatient before they would ever give it to me. They found a big ole ulcer in the process partially healed where they prescribed PrevAcid which is supposedly a acid pump inhibitor which nearly shuts off all your acid making ability (according to my GI specialist). It didn't impact my OSA any and I run reports regularly, but then mine look more like her 12/8 report than those prior.
I am still interested in learning how the acid reflux triggers these central events (that is a huge discovery in my opinion), what receptors is it may be influencing, that would be an interesting read.
Learn something new every day
Wow. What a blast from the past. Loonlvr's data looked an awful lot like Carla's: episodic NR's and AI increases. Some nights good and some nights bad. But what's more episodic: classic-etiology apnea that moist of us have or acid reflux? The answer is acid reflux flareups are much more episodic than garden-variety apnea. Loonlvr's treatment of his episodic acid reflux made his episodic bad AI/NR nights magically go away.Rested Gal wrote:Please re-read this:
viewtopic.php?t=5551
Snoredog, you asked about what obstructive-apnea etiology may be at play regarding acid reflux. To this day modern medicine has yet to arrive at a consensus opinion on that one. Interestingly, though, if you review somewhat older medical literature about vocal chord dysfunction (VCD), you'll see plenty of references to acid reflux being a chronic VCD trigger. And you'll also see references among many of those specialists that VCD patients can be nocturnally VCD, and therefore apneic with that VCD etiology.
All the while VCD specialists were propagating the above information, main stream sleep medicine largely failed to embrace the findings and opinions of those VCD specialists. And yet, at the same time, you could also find some mainstream sleep specialists theorizing that acid reflux just may cause vocal chord spasms and hence obstructive apneas in patients with these two comorbidities. Go figure! In my opinion that's a sure sign that sleep science is a very young branch of medicine. Quite understandable in my opinion as well, however.
But what about those NR events? My opinion is that in many cases 20 or even 25 water column of pressure may not open spastic and/or defensively closed vocal chords. Now Carla tells us that she has terrible aerophagia. And in my way of analyzing that implies terrible lower esophageal sphincter (LES) closure. And terrible LES closure is usually a two-way street. Meaning that Carla is probably at higher risk of acid reflux issues, because of that poor LES closure that likely results in here problematic aerophagia. And when Carla is supine, her compromised LES does not enjoy the same potential energy benefits of Gravity as when she is sitting or standing.
Night time acid reflux, episodically bathing those vocal chords. Episodic nights of high AI and occasional NR as well. Carla, I guess I too would suspect that it might not be a bad idea for you and your doctor to review the possibility of acid reflux as perhaps exacerbating your sleep apnea on an episodic basis. Most importantly, Carla, please remember that we're all wagering non-professional opinions and guesses. We simply can't diagnose. But we can give you ideas to discuss with your doctor(s). Good luck!
I won't go into my own theories about a "defensive physiologic bias" occuring in cases of VCD, CSDB, and a few other suspected etiologies. .
-SWS wrote:Wow. What a blast from the past. Loonlvr's data looked an awful lot like Carla's: episodic NR's and AI increases. Some nights good and some nights bad. But what's more episodic: classic-etiology apnea that moist of us have or acid reflux? The answer is acid reflux flareups are much more episodic than garden-variety apnea. Loonlvr's treatment of his episodic acid reflux made his episodic bad AI/NR nights magically go away.Rested Gal wrote:Please re-read this:
viewtopic.php?t=5551
Snoredog, you asked about what obstructive-apnea etiology may be at play regarding acid reflux. To this day modern medicine has yet to arrive at a consensus opinion on that one. Interestingly, though, if you review somewhat older medical literature about vocal chord dysfunction (VCD), you'll see plenty of references to acid reflux being a chronic VCD trigger. And you'll also see references among many of those specialists that VCD patients can be nocturnally VCD, and therefore apneic with that VCD etiology.
All the while VCD specialists were propagating the above information, main stream sleep medicine largely failed to embrace the findings and opinions of those VCD specialists. And yet, at the same time, you could also find some mainstream sleep specialists theorizing that acid reflux just may cause vocal chord spasms and hence obstructive apneas in patients with these two comorbidities. Go figure! In my opinion that's a sure sign that sleep science is a very young branch of medicine. Quite understandable in my opinion as well, however.
But what about those NR events? My opinion is that in many cases 20 or even 25 water column of pressure may not open spastic and/or defensively closed vocal chords. Now Carla tells us that she has terrible aerophagia. And in my way of analyzing that implies terrible lower esophageal sphincter (LES) closure. And terrible LES closure is usually a two-way street. Meaning that Carla is probably at higher risk of acid reflux issues, because of that poor LES closure that likely results in here problematic aerophagia. And when Carla is supine, her compromised LES does not enjoy the same potential energy benefits of Gravity as when she is sitting or standing.
Night time acid reflux, episodically bathing those vocal chords. Episodic nights of high AI and occasional NR as well. Carla, I guess I too would suspect that it might not be a bad idea for you and your doctor to review the possibility of acid reflux as perhaps exacerbating your sleep apnea on an episodic basis. Most importantly, Carla, please remember that we're all wagering non-professional opinions and guesses. We simply can't diagnose. But we can give you ideas to discuss with your doctor(s). Good luck!
I won't go into my own theories about a "defensive physiologic bias" occuring in cases of VCD, CSDB, and a few other suspected etiologies. .
-
curtcurt46
- Posts: 262
- Joined: Wed Sep 27, 2006 12:35 pm
- Location: Retired US Army
Dear Snoredog,
You just don't get it. I know how to read and in some cases put 2 and 2 together to get 4. You have latched on to an idea and can’t see some other possibilities. When I take the time to put something in the written form I do so from a most informed mind. To address your question first and then I will propose a question for you.
Snoredog wrote:
“Don't think so bud, where are you getting this variable breathing data?
This is a Remstar Auto it doesn't record variable breathing (VB), maybe if it was a AutoBipap it would, but not the Auto. Don't confuse variable breathing with erratic breathing after an event.”
Take a look at the auto- titration pressure support patent application, page 12-13.
http://lewiston.mit.edu/sleep/autopatent.pdf
Guess what, here is where I got this idea. MyEncore reports the variable breathing data for both auto bipap and auto pap. Variable breathing is a controller in both the Auto pap and the auto bipap. I am not confused, but I believe you may be. Give this a read and then tell me that data is not collected. Also look at Carla’s MyEncore reports and there you will find a whole page showing the VB for each day.
My reading tells me that variable breathing is an indicator of something out of order when the VB spikes above the average VB. I have seen this in my own data and now Carla’s.
Please tell me where the data is that supports that Carla has central apneas. You said there is a pattern, but I didn’t see it. Please show me where X+X+X= central apnea.
You just don't get it. I know how to read and in some cases put 2 and 2 together to get 4. You have latched on to an idea and can’t see some other possibilities. When I take the time to put something in the written form I do so from a most informed mind. To address your question first and then I will propose a question for you.
Snoredog wrote:
“Don't think so bud, where are you getting this variable breathing data?
This is a Remstar Auto it doesn't record variable breathing (VB), maybe if it was a AutoBipap it would, but not the Auto. Don't confuse variable breathing with erratic breathing after an event.”
Take a look at the auto- titration pressure support patent application, page 12-13.
http://lewiston.mit.edu/sleep/autopatent.pdf
Guess what, here is where I got this idea. MyEncore reports the variable breathing data for both auto bipap and auto pap. Variable breathing is a controller in both the Auto pap and the auto bipap. I am not confused, but I believe you may be. Give this a read and then tell me that data is not collected. Also look at Carla’s MyEncore reports and there you will find a whole page showing the VB for each day.
My reading tells me that variable breathing is an indicator of something out of order when the VB spikes above the average VB. I have seen this in my own data and now Carla’s.
Please tell me where the data is that supports that Carla has central apneas. You said there is a pattern, but I didn’t see it. Please show me where X+X+X= central apnea.
Curtis
curtcurt46
curtcurt46
Based on the 420e's central-apnea specificity rating of 100%: loonlvr's were, indeed, central apneas. That's what absolutely amazed us as we analyzed loonlver's data chart after data chart. His outstanding central and mixed apneas were amazingly just as episodic as his acid reflux flareups. Then, of course, both having abated with his acid reflux treatment. I have seen that pattern twice since, and now with Carla, perhaps a fourth time in total.Snoredog wrote:What are your thoughts as far as those actually being central events? We have the Remstar logging NR's and you know how that works, we have the 420e recording suspect Apnea/CA events as in loonlvr's and it has a pneumotach sensor. They are clearly gone in the 2nd report, same on Carla's 12/8 and I've seen the same on mine.
At the time there were no medical theories that I could find that would explain those strongly correlated central apneas paired with acid reflux flareups. At some point after analyzing loonlvr's response I started to suspect that this process was likely not a random, neurologically-driven vocal chord spasm. But that it was a defensive vocal chord closure orchestrated by neural adaptive plasticity. And if neural adaptive plasticity was defensively closing vocal chords, then neural adaptive plasticity was probably also defensively withholding breath in Loonlvr's case. Here you theoretically had defensive vocal chord closures (obstructive apneas) as well as defensive autonomic breath-holding (central apneas), both orchestrated by adaptive neural plasticity. And you also presumably had these two apnea phenotypes alternating and occurring in tandem, with mixed apneas thus resulting as well.
If, or perhaps better stated when, adaptive neural pasticity decides to defensively withhold breath, it will then balance the dilemma of two physiologic-based survival risks. It will decide, at least partially, on the basis of a heightened CO2 inspiratory target, when the risks of defensive breath holding outweigh the airway risks of an acid reflux episode. That is just my own theory, and it should not be tossed around as if it had any kind of medical credence whatsoever.
Your daughter finished dental school already? And now she's on to specializing in her profession? Aren't you a proud dad? .