Post
by avi123 » Tue Feb 11, 2014 9:18 pm
mellabella, if you have UARS then raising the XPAP pressure, most likely, would not treat it completely. Overall, an XPAP could help a little depending on what causes your UARS.
Clinical Features Associated With UARS
Daytime symptoms:
Excessive daytime sleepiness
Fatigue
Morning headaches
Myalgias
Difficulty concentrating
Sleep disturbances:
Frequent nocturnal awakenings
Difficulties initiating sleep
Insomnia
Bruxism
Restless leg syndrome
Unrefreshing sleep
Autonomic nervous system:
Hypotension
Orthostasis
Cold hands and feet
Functional somatic syndrome associations:
Depression
Anxiety
Chronic fatigue syndrome
Irritable bowel syndrome
Fibromyalgia
Polysomnographic abnormalities:
Increased RERAs
Increased nocturnal arousals
Increased CAP rate
Alpha intrusion during sleep
________________________________________
Treatment
[as of 2011]
The optimal treatment for patients with UARS is not currently known. Continuous positive airway pressure (CPAP) has been quite useful in the treatment of sleep-disordered breathing and there are some notable positive results in CPAP treatment of UARS. In a study of 15 heavy snorers with clinical evidence of UARS, treatment with nasal CPAP was associated with decreases in observed nocturnal arousals on polysomnography and decreases in mean sleep latency times on multiple sleep latency testing (MSLT) after several nights of treatment.3,36 A follow-up study of 15 subjects (in the original description of UARS) with daytime sleepiness and fatigue and who had undergone a therapeutic trial of positive pressure therapy reported similar findings.3 After treatment with approximately a month of nasal CPAP, significant improvements were seen in mean sleep latency times on MSLT (5.3 minutes vs 13.5 minutes), Pes nadir pressure (–33.1 cm H2O vs –5.3 cm H2O), amount of slow-wave sleep (1.2% vs 9.7%), and EEG arousals (31.3 vs 7.9 events/hour of sleep). Along with an improvement in sleep latency times on MSLT, there were subjective reports of improved daytime symptoms. Lastly, in a study of 130 postmenopausal women with chronic insomnia and evidence of UARS (n=62) or normal breathing (n=68), treatment with either nasal turbinectomy or nasal CPAP was associated with improvements in subjective reports of sleep quality as measured with a visual analog scale as well as mean sleep latency times on polysomnography.19 Despite the growing body of evidence supporting the use of positive pressure therapy for UARS patients, it remains difficult to obtain therapy. In a follow-up study of more than 90 patients conducted 4 to 5 years after the initial diagnosis of UARS was made, none of the subjects were receiving CPAP treatment; the main rationale given was that their insurance provider declined to provide the necessary equipment.1 Formal follow-up clinical evaluations of these patients noted significant worsening in their sleep-related complaints, with increased reports of fatigue, insomnia, and depressive mood. More disturbingly, prescriptions for hypnotics, stimulants, and antidepressants increased more than fivefold.
Other interventions, such as surgery or oral appliances, have also been used with some success in the treatment of patients with UARS. Procedures such as uvulopalatopharyngoplasty, laser-assisted uvuloplasty (LAUP), septoplasty with turbinate reduction, genioglossus advancement, and radiofrequency ablation of the palate have all been described in the literature.37-40 A study of LAUP in nine patients with UARS who underwent uvulopalatopharyngoplasty (n=2), multilevel pharyngeal surgery (n=1), or LAUP (n=6) reported improvements in subjective daytime sleepiness as measured with Epworth Sleepiness Scale scores.37 In the two patients for whom postoperative polysomnographic data was available, significant improvements in Pes nadir pressures were seen. But patients had several interventions and it is difficult to assess which one was successful. A study of 14 patients with UARS who underwent radiofrequency ablation of the palate also reported improvement in subjective sleepiness, with concurrent improvements in Pes nadir levels and reports of snoring.40 However, prior reviews of the available literature have noted that many of the studies evaluated small numbers of patients, consisted of uncontrolled case reports or series without clear characterization of the subjects enrolled, and had no consistent end points for an adequate evaluation of efficacy.39 Further investigation is required to determine the specific role for surgical intervention in these patients. Other authors have also reported successful treatment of UARS with use of oral appliances, although these studies suffer from the same limitations as the surgical literature.41 In children, orthodontic approaches, such as maxillary distraction or use of expanders, have also shown promising results.42
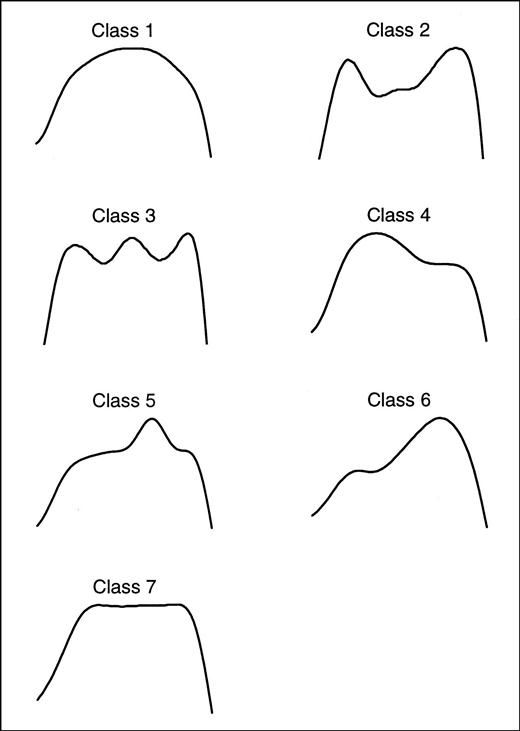
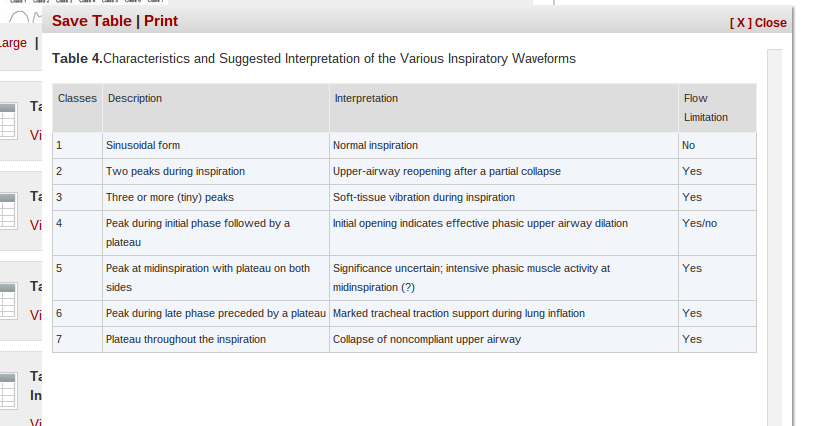
Conclusion
Although UARS has a symptomatology close to the one seen in patients with OSAS, there are distinct clinical differences between the two syndromes. In clinical studies, it is seen more in younger, slim subjects and in premenopausal women; it is more commonly associated with an increase in vagal tone during sleep than with sympathetic hyperactivity (as seen in association with apnea and hypopnea and oxygen desaturation).21 Can individuals with UARS become patients with OSAS? Guilleminault and colleagues1 suggested that weight increase (with development of a chest-bellow problem related to abdominal obesity) and the association of the supine position and sleep (leading to a restrictive impairment and secondary oxygen saturation drop and sympathetic hyperactivity) will lead to passage from one presentation to another with different complications; but more data are needed from additional systematic, longitudinal studies.1 UARS is underdiagnosed owing to unfamiliarity with the syndrome and the lack of polysomnographic criteria for either hypopneas or apneas that are associated with other types of sleep-disordered breathing. The advent of use of an esophageal catheter for esophageal pressure measurement (Pes) has allowed clinicians to more clearly identify patients with UARS. Although Pes measurement is the most sensitive method available to detect the abnormal respiratory events in UARS, it has not been used widely for several reasons, including lack of clinician experience and patient reports of discomfort. Usage of the nasal cannula pressure transducer allows recognition of flow limitation.43 But guidelines on how to tabulate the amount of flow limitation during total sleep time are lacking. Patients with UARS have significant impairment in their daytime functioning, with reports of sleepiness, fatigue, and sleep disruption. A follow-up study of these patients has shown that they often go untreated and experience progressive worsening of their symptoms. Among those patients who have been treated, typically with CPAP therapy, many have experienced symptomatic improvement. The current fund of knowledge regarding UARS has been growing, and we are beginning to understand the underlying pathophysiology.
________________________________________




















{kind=link}
{kind=link}
{kind=link}