RIC Wrote:
I'm not sure I understand what you meant about the data "looks so pretty and can be so wrong".
Ric also had a long discussion on how APAPs prevent events - which is close to what happens.
Here is the explanation of why the data can be wrong - and what happens in the modern machines.
I am sure that many of you have seen graphs of what a normal breathing cycle looks like, and probably some that show how the top of the waveform is clipped flat (flow limitaton) and other things.
The problem is that those are idealized "average" graphs. Real people vary from those ideals. Otherwise, building an APAP would have been ridiculously easy (and everyone's machine would work the same way).
So the Mfr takes their "Ideal" breathing pattern - as seen by the technology they chose to use to detect it (and there can be large variations in that).
Then they define what an "Ideal" snore, flow limitation, hypopnea, apnea, etc are and write a program to look for those "Ideal" patterns (depending on which of those they chose to use - no machine that I am aware of uses all "theoretically" detectable events).
Then experience has taught the Mfr's that you cannot respond to just one "event" - and that in most cases the response needs to be modest. So the Mfr determines how many of what kinds of "ideal" events have to occur before the machine will respond (at all) - and how fast (folks - there once were machines that would literally increase pressure so fast as to blow the mask off your face - waking you in the process - from the first indication of an event - and by false events indications such as rolling over or being jabbed by your spouse - or that "pregnant" pause when the dog licks your face in the middle of the night).
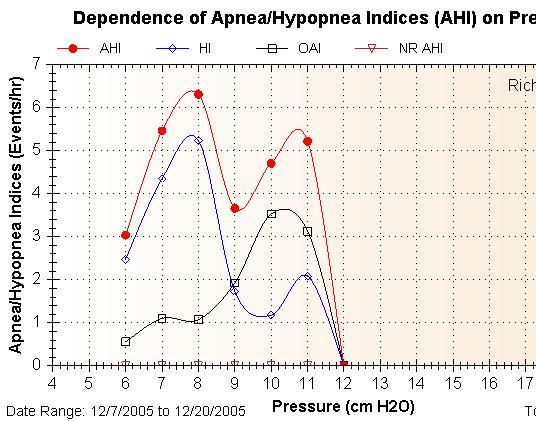
As you can see - even in the ideal case - the machine allows a certain number of events, and then in almost all cases slowly ramps up (allowing more). The idea is to get to a point where the "event rate" stops increasing and then to stabilize at a low event rate (and not wake you from too fast of a pressure increase). Then - after a predetermined amount of time determined by the Mfr the machine will reduce pressure. Should more significant events occur - increasing the event rate - the pressure returns to where it was - or even increases depending on the type of events and the rates.
Just to complicate things: In almost all cases - each Mfr has defined different "Ideal" breathing curves and different "Ideal" events - as they try to target what they think works best (if you would consider just a simple case - How would you define "snore" and how would you detect it...., then how would you respond to it - is some snore OK).
Of course, each person is different - and the key to how well any APAP works in auto mode (and the data collection in any mode) is how well the individuals personal breathing curve and personal event curves match what the machine is looking for. This can be great, good, fair, or bad.
The machine only records and responds to events that match what it has been told to record and respond to. That can be much different than what the person is actually experiencing. Hence the data output may or may not have a good correlation to the patient. In my example: Snore just right for the machine - and it's got a good precursor for you. Snore outside of the machines definition or detection capability - and the machine will report no snore.
This is why I challenge data with the simple test of is the person getting really good sleep treatment. An APAP that matches you well - and is setup properly (a separate issue) - should get a person to - or real close - to "mental zest" in a couple of weeks (or at worst a couple months)assuming that there are no other medical problems.
I can dig up Plenty of "good charts" out of my and other's personal experience alone where the APAP machine did not work for that person - did not allow them to get a good nights sleep. In my case: testing APAP machines from various Mfr's was really instructive - It really takes a masicist to do some of the things I have done - like repeating a 4 day multi-night test 3 times (after full recovery between test) with a machine that does not properly read me and respond to me - pushing me into exhaustion by day 3).
Now, truth be told - most people will do well on most any of the current APAPs. The problems are the people who's breathing and event curves are sufficiently far from "ideal" for that specific machine - as that machine is substantially missing the picture. The graphs look great - and the person is tired and miserable (and having real events that the machine does not see).
One of the advantages to having different Mfr's is that most likely a person can be adequately treated by one of the machines (since they all are actually looking for something different, even if the event shares a common name, - and respond at different rates).
Note however, there are people who's breathing and event patterns are sufficiently removed from the ideals that APAP will not work for them. There are also a number of other health issues that can prevent APAP from working. Of course, there are also a number of other health problems that a properly functioning APAP helps with (compared to CPAP).
Hope this helps (and yes, I know that I have probably created more questions than I answered. How APAPS work - under what conditions - etc is a long subject with a number of possible variables - I can't cover all of them in a few days).
I will be out of town tomorrow as I travel to visit a brother. Have a great Xmas.
Edited to add: If it seems that an APAP is not working that well for you - the first things to look for are proper set-up, mask leaks, and other health problems. Those charts often have other really interesting things in them for people who know how the machines sees, for example, asthma.
Perry
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition):
CPAP,
Hypopnea,
auto,
APAP,
Travel