NotMuffy wrote:jnk wrote:Funny thing is, sleep medicine finds itself in the awkward position of its testing costing much more than simply trying the treatment, too.
Your generalizations and syllogisms should add another 300 replies to this thread,
I admit it. I was trying to bait you into keeping the thread going. I am interested in your take on that "position"--help given by sleep docs who don't understand the technology.
I much prefer the way YOU have kept the thread going, though.
My worry is that sometimes patients think: "I need another sleep study to see if I'm having flow limitations so I can start treating THEM instead of just treating apneas and hypopneas." I think if they walk into a doc's office and say that, they are more likely to make a doc mad than to get any sympathy and action.
On the other hand, if they, as patients, walk into the same doc's office and say "I am still sleepy and tired and still wake up feeling like doggie-doo," they are much more likely to get help with an adjustment of pressure, a different machine, or a thorough examination of other health issues and sleep hygiene, etc.
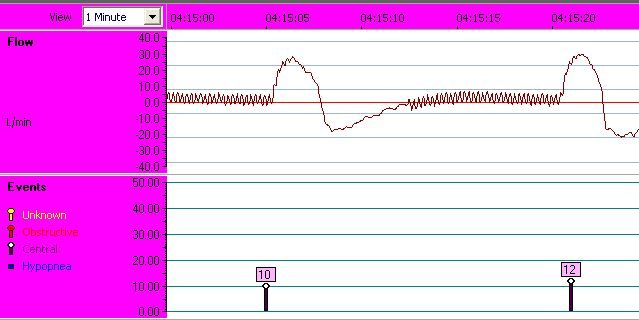
And if a patient walks into a doc with his S9 flow printouts to prove RERAs, the doc may be less than entertained by that, even though I have no doubt it could be done.
The kind of stuff you have posted in this thread is some of the most valuable stuff anywhere on the Web for patients with sleep problems, in my opinion. The help you provide to people like secret agent girl and others is some of the most amazing interaction I've seen occur anywhere, as far as being valuable to other patients and professionals who happen by here. What I appreciate most is that you not only explain things about the technology of the testing and treatments and the intricacies of how they can both be used to help patients but you also point out the broad overview and the various positions by researchers and practitioners. That kind of insight, experience, and perspective is very much appreciated.
That's why I stooped to baiting you. Not trolling. Just trying to do my part to keep you posting. It's a fine line for me sometimes. Sorry.