jnk wrote:the filtered brand will report less than the unfiltered one. Or is that just blowing smoke?
As in filtered/unfiltered cigarette smoke? Good play on words, jnk!
I haven't looked at the breath recovery issue yet. But I agree with what I
think your general point is: I happen to think the different brands necessarily entail a
variety of different design-judgments, regarding implementation specifics such as mean-flow data normalization, event scoring thresholds, and event discounting/filtering---especially in the midst of both baselining and temporal-variable trending adversities presented by highly erratic patient flow signals.
Or inversely stating my data view for the sake of an entertaining analytical paradigm shift: I agree that the manufacturers' proprietary HI scoring methods should yield far more similar HI outcomes during non-variant or less variable flow data moments---versus sustained periods of highly erratic flow data.
Those latter moments of wild data movement---when baselining attainability itself becomes highly challenged---are exactly when we
should expect maximum HI scoring disparity from differing proprietary methods.
_________________________________________________________________________________________________________________________
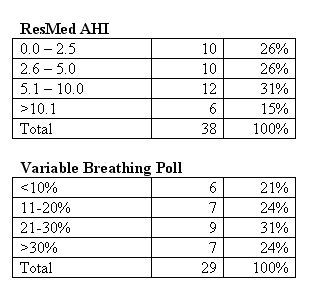
Muffy wrote:the relationship of rogue HI (AIs are constant and therefore need not be considered) to VB% is demonstrated:
<insert separate Resmed AHI and Respironics VB% survey results here>
...and the precise generalization can be made that the Variable Breathing Mode of the Respironics algorithm "weeds out" those artifactual hypopneas associated with "troubled wake".
When you get a chance can you explain to my pea brain how comparing a sample of Resmed AHI against yet a different and independent sample of Respironics VB% somehow statistically demonstrates that Respironics is discarding hypopneas during the wake stage?