




Why doesn't APAP respond to apneas?



Re: Why doesn't APAP respond to apneas?
You can bet on that.
Diagnosed 9/4/07
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1

Re: Why doesn't APAP respond to apneas?
PS - If anyone wants a copy of the Bipap AutoSV Provider manual it is here ...
http://www.internetage.ws/cpapdata/manu ... manual.pdf
DSM
http://www.internetage.ws/cpapdata/manu ... manual.pdf
DSM
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
Re: Why doesn't APAP respond to apneas?
Bev, the bad news is that you'll have to choose whatever suits your fancy.OutaSync wrote:So, are we agreed to try Snoredog's numbers for tonight? I don't do well with choices. I need specific instructions.
Snoredog's suggested settings actually sound pretty darn good to me. The main issue I have with that approach, however, is that if those settings work or don't work, we'll have a very hard time figuring out exactly which of those eight or so simultaneous changes contributed favorable deltas and which contributed unfavorable. We'll only see the sum-total end result of all changes that went into that night.
My own paradigm has always been to collect baselines for comparison... then to very methodically introduce one or few deltas so that each delta's good or bad contributions can be more easily discerned toward the final result. Despite that paradigm of mine, I have absolutely no problem whatsoever using Snoredog's "go-for-the-gold" shotgun approach!
Doug, thanks for posting that manual!
Re: Why doesn't APAP respond to apneas?
Bev, I would propose working up to Snoredog's suggested settings in two nights:
Snoredog, how does that two-pass approach sound to you? At the end of that second test you'll still get to see the sum-total result of your proposed changes.
Friday's Snoredog experiment wrote:EPAP=14
EPAP=14
IPAP Min=14
IPAP Max=18
Auto BPM
Rise Time 4 or 5
and take a melatonin
That two-pass approach allows us to introduce Snoredog's above proposed changes via two delta sets. That makes it just a bit easier to track some of those experimental deltas. The Auto BMP to manual BPM w/IT change is potentially very altering. And so is the CPAP@14+SV change. So I think it might make for easier tracking to separate those two deltas...Saturday's Snoredog experiment wrote:EPAP=14
EPAP=14
IPAP Min=14
IPAP Max=18
BPM=10
IT=1.2
Rise Time 4 or 5
and take a melatonin
Snoredog, how does that two-pass approach sound to you? At the end of that second test you'll still get to see the sum-total result of your proposed changes.
Re: Why doesn't APAP respond to apneas?
I agree. I thought it was a great idea - but that clearly didn't come through in my comment. By using the SV to track the variables we don't get on the regular machines, and keeping the setup without an SV, we'll be learning a lot about Bev's breathing under xpap when she's at home - and that's info we need.-SWS wrote:If SV is being trialed I sure would think that's a given----since that's the only data set capable of reporting PB and a few other parameters that haven't been comparatively scrutinized yet.ozij wrote:However, tracking any of those ways while using the SV's detailed reporting is an excellent idea.-SWS wrote: As always there are plenty of ways to skin a cat.
O.
Not that the data sets on the OSA machines are utterly lacking data. They're simply a different set of parameters---of which comparison thus far has yielded very little conclusion and daytime improvement. So yes.... using a data set with different parameters for comparison is potentially useful I would think.
But then again those tricky cats tend to have nine lives....
O.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Re: Why doesn't APAP respond to apneas?
Thanks for the manual, Doug.
O.
O.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023

Re: Why doesn't APAP respond to apneas?
Actually I don't want to see her in BPM=Auto at all. Using the settings below,-SWS wrote: That two-pass approach allows us to introduce Snoredog's above proposed changes via two delta sets. That makes it just a bit easier to track some of those experimental deltas. The Auto BMP to manual BPM w/IT change is potentially very altering. And so is the CPAP@14+SV change. So I think it might make for easier tracking to separate those two deltas...
Snoredog, how does that two-pass approach sound to you? At the end of that second test you'll still get to see the sum-total result of your proposed changes.
EPAP=14 cm (fixed CPAP at 14 cm, same as last night)
IPAP MIn=14
IPAP Max=18 (pressure support from 14 cm to 18 cm for SV mode working pressure)
Settings below are ONLY for backup mode, these settings are automatically set in SV mode:
BPM=10 (fixed mode)
IT=1.2
Rise Time=4 or 5
Reason I don't want to see her backup mode in BPM=Auto is:
-if the machine screws up in SV mode and goes out of control like we seen on night 2 and 3, I want her landing at known fixed state that will correct and slow breathing down.
-BPM or backup mode is ONLY used for control of central dysregulation.
If she lands in backup mode to fixed setting known to slow her breathing down (typical S/T settings), that slower breathing will carry over to the SV mode where 4 minute sampling again restarts and this time hopefully it will pick up a slower breathing rate and keep her from falling back into periodic breathing soon followed by central dysregulation.
Note: her 1st night SV Encore report showed BPM=14.6 in SV mode. She had no cycling to backup mode that night. I assume that is still a bit fast for her as her volumes we seen were a bit low for her height. So if we follow protocol for BPM, it would be spontaneous rate @14.6 -2 = BPM=12.6. So if I want to slow her breathing down when she lands at fixed BPM=12.6 that should ideally do it, but if centrals are present a lower setting of BPM=10 and IT=1.2 will surely eliminate any centrals IF she lands there.
So I only support the above fixed settings (IPAP is still Auto in SV mode). If this machine's Auto mode was a panacea we wouldn't be seeing the patient cycling over to backup mode. It should be controlling her breathing to avoid any central dysregulation and the backup modality IMO.
In other words, it is my belief this machine is:
1. Sampling her Spontaneous breathing which is already too fast and applying those avg values to BPM=Auto. My example given to DSM the other
day was if a patient had a RR=18 and machine applied its manual protocol values to this via the SV algorithm, that patient with RR=18 would only be at 16 in Backup Mode (BPM=Auto), still too fast. This backup rate of BPM=16 will most likely still too fast. The result is unnecessary cycling to backup mode which doesn't slow breathing enough. Known "Fixed" settings do.
2. I see success with this machine measured by:
-elimination of all obstructive events (accomplished by EPAP)
-elimination of Periodic Breathing (accomplished by PS IPAP Min to IPAP Max and SV algorithm)
-elimination of Central Dysregulation (avoiding PB, and backup mode).
-100% Patient triggered breathing
So it is my belief (and opinion) this machine uses backup settings carried over to spontaneous mode. If it is doing its job in the Spontaneous or SV mode, the patient should never cycle to the backup mode.
I find the introduction of PB (Periodic Breathing) very troubling and should be avoided at all costs. When a patient goes into Periodic Breathing they tend to hyperventilate (short rapid breaths), they can increase or double their RR which only exhausts more CO2 out, which is why central dysregulation soon follows. If I want you to retain more CO2 I simply stop you from breathing.
So if the machine's "auto mode" screwed up in SV mode I see no reason to reward it by allowing it to screw up back up mode. Obviously this is from us finding initial settings.
It is also my belief that BPM=Auto is for only finding those initial parameters needed to establish fixed settings for backup mode, once it is learned that obstructive events are taken care of and RR stable, those settings are transferred to fixed backup settings. Why else would the mfg call for using Spontaneous settings -2 for BPM mode? Obviously you cannot do that without knowing what they are, so Auto is for finding that.
BPM=Auto might work about as well as sending a patient home with an auto machine set 4cm to 20cm, it will work just not very good.
We all have our opinions on this machine, but I see it as follows:
CPAP, this is EPAP settings, designed to eliminate all obstructive events
SV, targets peak (inhale) and tidal (exhale) volumes to control Periodic Breathing
Backup Mode, fixed settings to slow patients breathing where they retain more CO2.
Day 1: To determine if EPAP=9 eliminated all obstructive events (it did).
Day 2: Increase in Minimum Pressure Support resulted in first introduction of PB and cycling to backup mode (settings produced Central dysregulation).
Day 3: Same settings used, more Periodic Breathing and cycling seen and worst results. Now I know the machine responded correctly to the PB but that is not the point, it took only 1 cm of Pressure Support to produce that result.
Day 4: Patient goes back on AFlex, basically CPAP at 14 has much better result than SV.
Day 5: Straight CPAP similar results as Aflex but more OA events seen, those events suspect as being "central" and recorded by machine as "obstructive".
someday science will catch up to what I'm saying...
Re: Why doesn't APAP respond to apneas?
yep, and its the very reason I don't make it a habit of doing this via PM's.-SWS wrote:I'm positive that I'm not the only one comforted and relieved that SAG is keeping tabs on this thread. Thank you SAG.
When done via PM's, No one learns from the discussion, any suggestions made aren't scrutinized or fall under the scrutiny of others who might know better.
so for the person receiving those suggestions, they get much better advice via the public forum. Sure it leads to arguments now and then but for the person getting the advice they are much better off.
someday science will catch up to what I'm saying...
-
StillAnotherGuest

- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
What Are You Fixing?
I think the next experiment should be to stop experimenting.OutaSync wrote:I'm ready for my next experiment. What shall I try next?
I remain in the camp that says the EDS is due to another cause(s).
Despite lacking current NPSG data (SDB under good control and medication-free), I believe Bev has significant Wake/Sleep transition issues.
SV technology hates Wake/Sleep transitions.
Even if that were not the case, there is no data from the current "experiments" to justify "central dysregulation" (2 salvos of events does not "central dysregulation" make. And since it takes a while to break the cyclical nature of "central dysregulation", despite driving thru those salvos with an SV attack, it is unlikely that they would actually be corrected. There is a difference between "driving thru" "central dysregulation" with a rate-controller and actually correcting it)(which I don't think the 1.3 version can differentiate)(determining that is on my list of "to do" things, but right now, it's a big list)(and most of it has nothing to do with work)(now where was I?)(oh, yeah)....
The AHI on CPAP 14.0 cmH2O is 1.4.
The AHI on CPAP 14.0 cmH2O is 1.4.
The AHI on CPAP 14.0 cmH2O is 1.4.
The AHI on CPAP 14.0 cmH2O is 1.4.
The AHI on CPAP 14.0 cmH2O is 1.4.
The AHI on CPAP 14.0 cmH2O is 1.4.
The AHI on CPAP 14.0 cmH2O is 1.4.
The AHI on CPAP 14.0 cmH2O is 1.4.
Wild Speculation
Now Lexapro-free, it's a good bet Bev now has REM. The first salvo of events occurs at 90 minutes. That would normally also be about the time of the first REM period, which would suggest REM-dependent OSA, not properly addressed by CPAP 14.0 cmH2O. (However, that does not completely rule-out the possibility of SOREM, either. You only need one "REM" to have a SOREM). If the first salvo is REM-dependent OSA, then it's 5-to-1 the second salvo is, too.
At this point, there appears to be a huge discepancy of NPSG titration results (which certainly do make a case for CSDB) and current data. Or, simply, it just took a while to "settle in", and the tendency to "overshoot" (reread the "loop gain" thing) has now resolved.
Conclusion
I think you guys are trying to shove a square peg into a round hole.
SAG
PS - You're welcome, Bev. Who would have thought that rewriting the firmware was that easy?

Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
Re: Why doesn't APAP respond to apneas?
Hmmmm,
Does my machine's 1.2 version do it better ???
(or perhaps worse )
By the way, what was the purpose of asking for the software version # ???
DSM
Does my machine's 1.2 version do it better ???
(or perhaps worse )
By the way, what was the purpose of asking for the software version # ???
DSM
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
But It Wouldn't Really Help...
If you want to do that, then you should change that line to read
But I think that would academic. If it responds, then by definition those events would be there, and they still won't differentiate.
SAG
Code: Select all
for f if n>0 then [list = event 0,1]SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
This Works
OK, use
They'll all be on the same line, but be different colors.
SAG
Code: Select all
event 0 = color#0013
event 1 = color#0075
for f if n>0 then [list = event 0,1]SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Right!
Exactly! The software can't read what the firmware don't write.
SAG
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
Re: Why doesn't APAP respond to apneas?
Since I went to bed before I saw SWS, Ozij and SAG's responses, I used Snoredog's suggestion and this is the result:
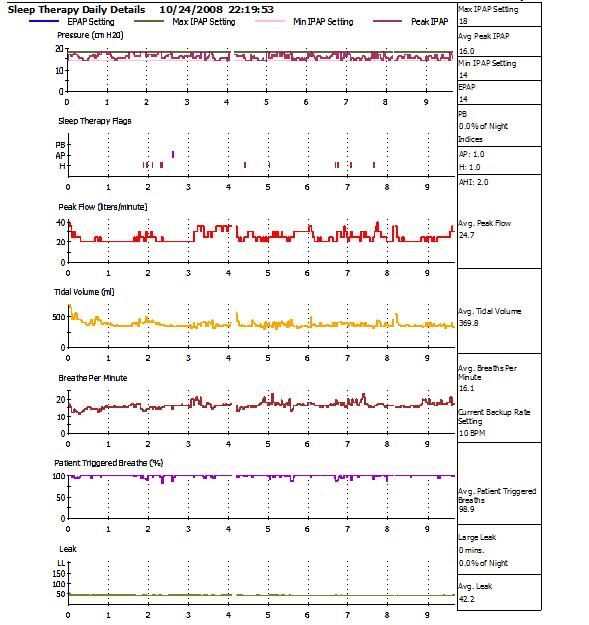
It took me awhile to get to sleep, even with the melatonin and the Ambien. There were a few times when the machine puffed at me when I wasn't finished exhaling. I had to get up a couple of times to let the air out of my stomach, and woke up with a headache.
Bev
It took me awhile to get to sleep, even with the melatonin and the Ambien. There were a few times when the machine puffed at me when I wasn't finished exhaling. I had to get up a couple of times to let the air out of my stomach, and woke up with a headache.
Bev
Diagnosed 9/4/07
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Re: Why doesn't APAP respond to apneas?
Thanks for the firmware dump SAG. The colored event types mentioned are PB, AP, and H. Those returned values apparently write to event-reporting data structures we see represented in the multicolor Encore graphs. Great to see that.
Bev, would you mind grabbing those two baselines on the AutoSV? One was to get recordings at 14cm CPAP and the other was to get recordings at 17/14 cm BiLevel.
Snoredog, I disagree entirely about turning Auto BPM off that early.
Bev, would you mind grabbing those two baselines on the AutoSV? One was to get recordings at 14cm CPAP and the other was to get recordings at 17/14 cm BiLevel.
Snoredog, I disagree entirely about turning Auto BPM off that early.