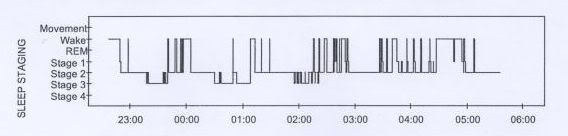
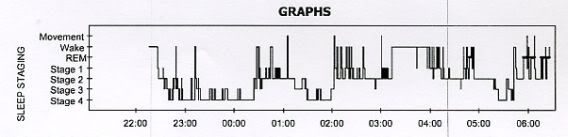
I absolutely agree that the pressure chairs occur in response to incessant little flow variations from Bev. But look at that left-most chair. It's not chair shaped. It's actually shaped like the Empire State Building, and King Kong is sitting on top of it----waiting to devastate that sleep architecture by angrily hurling RDI sleep disturbances across that nocturnal landscape.Snoredog wrote: SWS: see Bev's latest Encore report, notice how the little chairs change when an event is detected, notice her AHI even went down further to .8 (Bev you can stop trying to lower your AHI now )
One of the potential problems that SAG wanted to look for on Bev's PSG discs was the presence of alpha wave intrusions. He just may spot other interesting clues relevant to Bev's sleep architecture as well. Also, ozij may know something about Lexapro's possible long-term effects. I haven't completely dismissed Lexapro's potential role in this sustained sleep architecture mess either. Not by a long shot.
...By the way, I'm right back to thinking Bev's BiPAP AutoSV really needed to have its EPAP set at 14 cm:
That's exactly what I think may be happening in Bev's case with the autoSV's EPAP set too low. The end result is that IPAP peak uncomfortably throttles up and down near IPAP max for extended periods as we see on the SV charts.Stephen E. Brown, MD, DABSM wrote:In another patient, undertitration occurred as the technologist adjusted the EEP for apneas and hypopneas, but did not adequately increase the pressure for residual RERAs.
I think she probably has a narrow airway that simply needs more constant dilation via EPAP at 14 cm. That constant EPAP dilation may keep the IPAP peak activity from running into an apparent vicious cycle of: 1) very rapid airway inflation (via a huge EPAP/IPAP peak gap), 2) a counterproductive (pressure-variation) stimulus/response reaction from Bev, followed by 3) an even more aggressive and counterproductive IPAP peak "countering response" from the BiPAP autoSV. That third step conceivably brings Bev back to (neurologically reactive) step two in that incessantly repeating vicious cycle.
She conceivably needs EPAP's constant airway dilation right up there at the same 14 cm that yielded satisfactory results in the lab and at home on APAP. Then SV can take a more refined approach at straightening out those flow-amplitude variations with a bit more finesse and hopefully greater comfort.