






Tolja.... Fat ticks cause even more Lyme disease.
O.
Question on apap
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
-
StillAnotherGuest

- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
When You're Right, You're Right!
LOL! Yes, you did!ozij wrote:Tolja.... Fat ticks cause even more Lyme disease.
O.
I got another one where 420E misses EVERYTHING! And I mean everything!!
Lemme run the PSG part thru a few things...
SAG

Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
Guest
Hey there, O!ozij wrote:Hi there, -SWS!
Okay. Not to confuse data sampling rate (which occurs at the same rate in both machines) with graphical reporting. In general sampling rate potentially skews the specificity or sensitivity of instrumentation, but clinician's graphical reporting alone cannot. But reporting software can be highly erroneous as we all know.ozij wrote: I was thinking of that too - and when they changed from a 30 second sampling (418P) to a 60 second sample (420E)- it became an even rougher guide. But again, I agree - extremely helpful.
When we put those tick marks under close scrutiny, then we probably attempt to extract informational details that were never intended for those tick marks. Take examples of concurrent hypopnea and apnea tick marks, for instance. When we see those, we are probably seeing discrete sleep events in a very small epoch of time. They get graphically "scrunched up" to the point of being on vertical alignment. That's probably more of a white-space real estate issue than it is a reporting error. And it's certainly not a case of a hypopnea and apnea occurring simultaneously.
With that said, the overall reporting methodology (or tick mark layout) is probably best deciphered from many graphs with sparse but unique event distributions. Any given graph with an overly-dense distribution is likely to represent the issue of "graphically outstripped" white space.
I think you've missed my points about the caveats of processing acoustic signals (those caveats are not relevant to the low-velocity signals). Please note the quoted patent text I have underlined above. I think that's where your signal-processing oversight lies. At that point in analyzing the patent text we need to back up and ask ourselves if we have nicely preserved or inadvertently deteriorated the acoustic signal (cardiac oscillations here).SAG wrote:What this suggests to me is that if 420E sees an event, and that event has respiratory frequency-based waveform activity that is <10% of the previous 2 minute analysis window, and the event is at least 10 seconds long plus five-eighths of the average of the preceding three breaths, and then it finds cardiac frequency (40-120 cycles/minute) waveform activity, then it will call that an ApneaCA. Consequently, the speed of waveform transmission becomes academic.
So Laura scored plenty of 420e central apneas only on the night you substituted the argyle tube. Your tubing substitution clearly had acceptable low-velocity airflow characteristics, but it probably distorted the cardiac oscillation signals (that night only) because of an acoustic impedance mismatch.
The speed-of-sound issue is highly relevant. It is relevant because sound is one of the signal velocities at which transmission-line physics becomes essential. The low-velocity airflow signals simply do not suffer appreciable deterioration because of highly irrelevant acoustic-impedance mismatches. But speed-of-sound signals (especially subtle ones like cardiac oscillations) can become readily degraded by acoustic-impedance mismatches. In other words, if we're going to induce and then signal-process that cardiac-oscillation signal, then we are liable to the kinds of signal deterioration issues unique to speed-of-sound velocities.
Acoustic signal velocities are entirely central to whether we have preserved or deteriorated the signal because of an acoustic impedance mismatch. When there is an acoustic impedance mismatch then these two signal-distorting effects will occur: 1) the final or resultant cardiac oscillation signal (during non-apneic moments) will be reduced--making that acoustic signal very difficult to algorithmically normalize and baseline, and 2) during purely obstructive apnea moments (when there should be no appreciable cardiac oscillation signal present) you can have a false signal echo literally traveling traveling up and down that transmission signal line.
Do you see how the speed-of-sound is entirely central here? It's central to whether you have preserved or screwed up the acoustic signal. If you've observed speed-of-sound transmission-line physics, then you have preserved the delicate acoustic signal in question. However, if you neglect transmission-line physics, then you can easily screw up the cardiac oscillation signal itself---- to the point of generating false positives for central apneas (with bad acoustic signal signal baselining in the first place, followed by false signal echoes being present during obstructive moments).
The above is from the patent. Now, I never studied physics in English, and what physics I studied was long ago. So I may be all wrong. But the way I understand this is that the amplitude of the flow is oscillating at the rate of human heartbeat - defined by PB as 40-120.the pressure waveform is examined for cardiac oscillation at step 76, i.e. regular, small-amplitude flow pulsations with a frequency in the range of the cardiac frequency
I remember nights when I started therapy when I could hear the airflow chaging according to my heartbeat, a kind of "pffff, pffff, pfff". Which is why I said "camels dancing or limping". Not the sound of my heart, but the way my heartbeat physically changed the amplitude of the flow.
Do you mean, -SWS, that the info about this amplitude oscillation was affected by the Argyle tube ?
O.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): 420E
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
Last edited by ozij on Thu Nov 15, 2007 11:04 am, edited 1 time in total.
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Dieing of curiosity
SAG,
If its not too much trouble, can you export that *.pat file you have for CLFDS (aka RG) to ascii, and then take a look at the *.SE file at the relevant session to see how may hypopneas are reported?
O.
If its not too much trouble, can you export that *.pat file you have for CLFDS (aka RG) to ascii, and then take a look at the *.SE file at the relevant session to see how may hypopneas are reported?
O.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Signal amplitude speaks of the height/magnitude of the signal. Amplitude directly corresponds to how strong or faint the signal is. Frequency, of course, refers to cyclic repetition over time. Both parameters--amplitude and frequency--are essential to correctly processing this signal. When you see the patent text refer to a "small amplitude" flow pulsation, they are essentially saying that this signal is a relatively faint acoustic signal. That low signal amplitude, of course, makes the signal harder to baseline and subsequently measure/score when you generate signal reflection by mismatching acoustic impedances (the sensor's acoustic impedance versus the signal line's characteristic acoustic impedance in this case).ozij wrote:The above is from the patent. Now, I never studied physics in English, and what physics I studied was long ago. So I may be all wrong. But the way I understand this is that the amplitude of the flow is oscillating at the rate of human heartbeat - defined by PB as 40-120.the pressure waveform is examined for cardiac oscillation at step 76, i.e. regular, small-amplitude flow pulsations with a frequency in the range of the cardiac frequency
I cannot be sure, since we don't know the characteristic acoustic impedance of either tube. But if the argyle tube had a significantly different characteristic acoustic impedance compared to the original sensor line... then, indeed, the cardiac oscillation signal would have been amplitude-skewed (diminished during an ongoing baselining process) as well as being physically present on the signal line when it shouldn't have (as a faint signal echo during obstructive apneas---resulting in those false positives for central apneas).Ozij wrote: Do you mean, -SWS, that the info about this amplitude oscillation was affected by the Argyle tube ?
It's a very plausible explanation. But it hinges on whether the characteristic acoustic impedance was significantly out-of-spec for the argyle tube.
Right. That is not at all "front-end" data sampling. Front-end data sampling largely affects sensitivity, specificity, and even treatment (other issues do as well). Rather, what you see described here a a back-end process of finally getting around to reporting past-results to the clinician's software. That latter back-end reporting process doesn't impact the machine's detection or treatment algorithms regarding sensitivity or specificity.OziJ wrote: Re the sampling:
Silverlining's 420e manual says of the "detailed record": This screen analyzes the last 96 hours of operation including the recording of pressure (every 60 seconds).
Not to say that APAP machines process signals or sleep events perfectly. Of course they don't.
Ok, I think I got that re the tube - thanks.
I see you responded before I edited out the part of my post about the samplng...
I edited my comment out because I reread that part of the manual, and wanted to check something.... the manual is clear about reporting the pressure every 60 seconds - but on second thought I'm not so sure how they handle the event reporting.... It doesn't make sense for events to be sampled once a minute.... too rough.
O..
I see you responded before I edited out the part of my post about the samplng...
Yes, that it clear to me, detection and therapy can be independent of the reporting.Right. That is not at all "front-end" data sampling. Front-end data sampling largely affects sensitivity, specificity, and even treatment (other issues do as well). Rather, what you see described here a a back-end process of finally getting around to reporting past-results to the clinician's software. That latter back-end reporting process doesn't impact the machine's detection or treatment algorithms regarding sensitivity or specificity.OziJ wrote:
Re the sampling:
Silverlining's 420e manual says of the "detailed record": This screen analyzes the last 96 hours of operation including the recording of pressure (every 60 seconds).
I edited my comment out because I reread that part of the manual, and wanted to check something.... the manual is clear about reporting the pressure every 60 seconds - but on second thought I'm not so sure how they handle the event reporting.... It doesn't make sense for events to be sampled once a minute.... too rough.
O..
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
This Part?
You mean this one?ozij wrote:If its not too much trouble, can you export that *.pat file you have for CLFDS (aka RG) to ascii, and then take a look at the *.SE file at the relevant session to see how may hypopneas are reported?
Code: Select all
File : C:\SL3\Patient\Oct19-2005StudyNight.pat
Start date : 10/19/2005
End date : 10/19/2005
Period : 1days
Used pressures (Average) :
Average pressure : 9.0 cmH2O
Low pressure : 8.0 cmH2O
High pressure : 11.0 cmH2O
Pressure efficient more than 90% of time :10.0 cmH2O
Events :
Number Apneas : 4
Index/h Apneas : 0.6
Number Apneas/CA : 14
Index/h Apneas/CA : 2.1
Number Hypopneas : 36
Index/h Hypopneas : 5.5
Number Acoustical Vib. : 22
Index/h Acoustical Vib. : 3.4
Number Runs (FL): 151
Index/h Runs (FL): 23.1
Cycle states :
Normal cycle : 80 %
Intermediate cycle : 2 %
Flow Limited cycle : 17 %
Invalid cycle : 1 %
Last settings of the period :
( 0 setting change )
Mode : Pilot : A+AV+IFL2
Min. pressure : 8.0 cmH2O
Initial pressure : 8.0 cmH2O
Max. pressure : 14.0 cmH2O
Max. press. for command on Apnea : 10.0 cmH2O
Ramp duration : 0 min
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
I Think It's OK...
OK, if we can agree that it is correct to assign 1, 2, 3 and 4 events based on the width of the ticks, then in the 30 minute block from 86.5 to 87.0 there are 3 Apneas and 17 hypopneas. Of those 20 events, 15 have associated cardiac oscillations. Most importantly, hypopneas can have associated ApneaCAs.
The NPSG results in that period show 20 hypopneas, but several are easily close enough to be called apneas (depending on what Evolution calls an apnea. I've seen some references say "no flow", the patent suggests 90% reduction, but regardless, the Percent of Agreement is acceptable by Standard).
The remaining question concerns the presence of cardiac oscillations in the events. Looking at the last hypopnea in the 30 minute block, we see fairly clear oscillations:

So at this point, I don't see anything wrong with the way the 420E called those events.
What Difference?
Further, the other explanation offered (a kinked tube) seemed unlikely in that the effect on the waveform would be a dampening, thus reducing cardiac oscillation amplitude and their consequent identification by 420E. Certainly, it wouldn't increase amplitude, which would have to occur in order for the 420E to start sending out ApneaCAs.
Lastly, as was pointed out in the algorithm, and what I needed to do to generate the cardiac oscillation waveform, the signal at that point in the algorithm needs to be amplified, and a fair amount at that. Any artifact is also amplified, and the clarity of the CO signal would become obscured in the artifact (the concept of "signal-to-noise" ratio). Amplifying junk simply becomes amplified junk, yet the 420E events as scored are absolutely in keeping with the events in the PSG.
SAG
The NPSG results in that period show 20 hypopneas, but several are easily close enough to be called apneas (depending on what Evolution calls an apnea. I've seen some references say "no flow", the patent suggests 90% reduction, but regardless, the Percent of Agreement is acceptable by Standard).
The remaining question concerns the presence of cardiac oscillations in the events. Looking at the last hypopnea in the 30 minute block, we see fairly clear oscillations:
So at this point, I don't see anything wrong with the way the 420E called those events.
I had originally considered the possibility of the Argyle bubble contaminating the waveform when the events were first presented and tested that theory with a really outlandish length of bubble tubing pitted against a short length of standard 420E tubing, and there was no discernible difference:-SWS wrote:At that point in analyzing the patent text we need to back up and ask ourselves if we have nicely preserved or inadvertently deteriorated the acoustic signal (cardiac oscillations here).
What Difference?
Further, the other explanation offered (a kinked tube) seemed unlikely in that the effect on the waveform would be a dampening, thus reducing cardiac oscillation amplitude and their consequent identification by 420E. Certainly, it wouldn't increase amplitude, which would have to occur in order for the 420E to start sending out ApneaCAs.
Lastly, as was pointed out in the algorithm, and what I needed to do to generate the cardiac oscillation waveform, the signal at that point in the algorithm needs to be amplified, and a fair amount at that. Any artifact is also amplified, and the clarity of the CO signal would become obscured in the artifact (the concept of "signal-to-noise" ratio). Amplifying junk simply becomes amplified junk, yet the 420E events as scored are absolutely in keeping with the events in the PSG.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
Okay. I never followed this story too closely until now. I just took a very quick peek at your TAS post. Up until now I thought there was an issue with the 420e scoring central-apnea false-positives that Laura's same-night PSG did not score.SAG wrote:...yet the 420E events as scored are absolutely in keeping with the events in the PSG.
If those two "quantitative returns" are in agreement, then I don't think either instrumentation-set scored false-positives for central apneas. Or stated a different way: I don't think both instrumentation sets identically returned false-positives for central apneas.
I wonder if Laura's pre-PSG comment, "Pssst... watch me fake a few central apneas over at Dave's sleep center", had anything at all to do with this...
This part?
Thanks,. but not that one.
No, I meant what you get when you export from the detailed record screen; That export creates 3 additional files (detailed data per session (*.se), detialed data per 24 hours, (*.24h) and a detailed leak and pressure summary for the last 96 hours (*.96h).
I thind the apnea and hypopnea detials on the *.se file will be different from those we saw till now.
I import the files into Excel, the separator is a semi colon.
O.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): Hypopnea
No, I meant what you get when you export from the detailed record screen; That export creates 3 additional files (detailed data per session (*.se), detialed data per 24 hours, (*.24h) and a detailed leak and pressure summary for the last 96 hours (*.96h).
I thind the apnea and hypopnea detials on the *.se file will be different from those we saw till now.
I import the files into Excel, the separator is a semi colon.
O.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): Hypopnea
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
OK, Artful Dodger...
OK, I see that button.ozij wrote:No, I meant what you get when you export from the detailed record screen; That export creates 3 additional files (detailed data per session (*.se), detialed data per 24 hours, (*.24h) and a detailed leak and pressure summary for the last 96 hours (*.96h).
Hmmm. I'm gonna hafta import it to "Notepad", and separate it with an axe.ozij wrote:I import the files into Excel, the separator is a semi colon.
How can that be, it looks like the same routine as the other report I sent you:ozij wrote:I thind the apnea and hypopnea details on the *.se file will be different from those we saw till now.
Code: Select all
File : C:\SL3\Patient\Oct19-2005StudyNight.pat
Start date : 10/19/2005
End date : 10/19/2005
Events :
Number Apneas : 4
Number Apneas/CA : 14
Number Hypopneas : 36
Code: Select all
File : C:\SL3\Patient\Oct19-2005StudyNight.SE
Apneas: 1
Apneas/CA: 14
Hypopneas: 36
OK, whadya do with them other 3 apneas?
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
My Point Is...
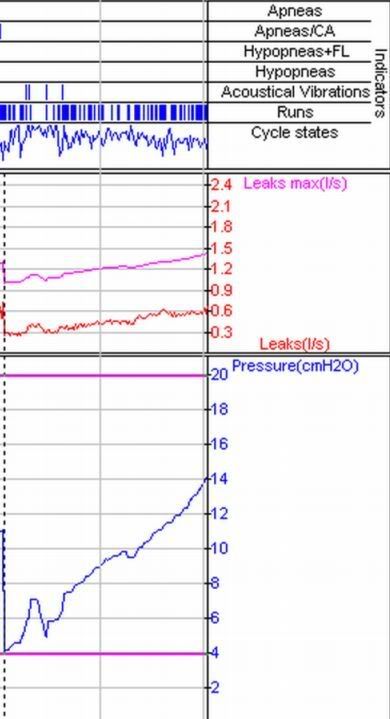
In all fairness to APAP algorithms the world 'round, it might be more appropriate to call this a design "limitation". The point of this one and RG's is that if you're trying to do diagnostics with single-channel data acquisition, there is a percentage of patients where major underlying disease states will be missed.-SWS wrote:No events measured... or no pressure combined with no events measured?SAG wrote: I got another one where 420E misses EVERYTHING! And I mean everything!!
So far this one sounds like a malfunction versus design shortcoming.
Submitted for your approval-- one strange APAP response:
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
Re: My Point Is...
In the "this one" screenshot of a two hour session... the person using a range of 4 - 20. Was IFL1 on?StillAnotherGuest wrote:The point of this one and RG's is that if you're trying to do diagnostics with single-channel data acquisition, there is a percentage of patients where major underlying disease states will be missed.
Submitted for your approval-- one strange APAP response:
SAG
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435