






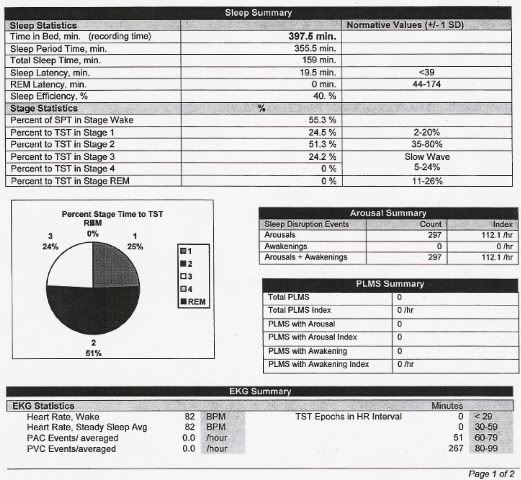
Last week's average:
AHI 2.9
OA 2.4
HI 0.5
SI 0.1
FLI 1.1
Opinion please - questions

Re: On Various Issues
StillAnotherGuest wrote:While it may be tempting to attribute sleep disturbance to SSRI administration, there are significant dangers inherent in doing so. You really have to know what the sleep architecture was prior to the initiation of anti-depressant medications before you can blame ADMs for sleep disorders. The incidence of insomnia in untreated depression is somewhere from 50-90% depending on who you talk to. For the sake of comparison, the incidence of insomnia attributed to SSRIs (depending on which one you pick) tends to be in the 20% range. The point is that the likelihood of insomnia being co-existent with depression is stronger than it is being as a result of ADM administration alone.
Understanding this co-morbidity makes understanding the pharmaceutical company-supplied brochures a little bit easier to explain. While the incidence of insomnia is often presented as being present in a comparatively large percentage of patients, the percentage of patients experiencing insomnia receiving placebo is also noted to be relative significant. Looking at Prozac and Effexor:
Prozac
Anxiety and Insomnia — In US placebo-controlled clinical trials for major depressive disorder, 12% to 16% of patients treated with Prozac and 7% to 9% of patients treated with placebo reported anxiety, nervousness, or insomnia.
In US placebo-controlled clinical trials for OCD, insomnia was reported in 28% of patients treated with Prozac and in 22% of patients treated with placebo. Anxiety was reported in 14% of patients treated with Prozac and in 7% of patients treated with placebo.
In US placebo-controlled clinical trials for bulimia nervosa, insomnia was reported in 33% of patients treated with Prozac 60 mg, and 13% of patients treated with placebo. Anxiety and nervousness were reported, respectively, in 15% and 11% of patients treated with Prozac 60 mg and in 9% and 5% of patients treated with placebo.Now, I don't know if their point was to say, "See, you got insomnia anyway" and they were just trying to do some damage control, or the incidence of insomnia-related ADM adminstration is significant, or perhaps, better yet, one should have a real good idea of sleep status prior to the initiation ADM therapy. Which, if you're here at this site, you have a concurrent issue that really complicates the mix and at this point really have no idea which entity is doing what.Effexor
On the other hand, I don't think you have to dig very far to discover that ADMs can significantly affect sleep architecture (and this includes sleep fragmentation as well as insomnia, which are 2 different things). But you have to be real careful about how much you rob Peter to pay Paul.
Also, don't forget that sudden or arbitrary withdrawal of ADM can result in significant issues, including the SSRI Withdrawal Syndrome. So don't think that you can self-titrate ADMs using Antidepressant 1.6 and MySSRI (but if you do, just make sure you load up the software first).
The Following Is A Paid Political Announcement
One more thing. I'm really looking forward to the day when unattended portable screening for OSA becomes commonplace, and patients with issues like these wallow aimlessly around with undiagnosed co-morbidities. Without an exceptionally good screening tool and qualified people to administer it (which in practice, absolutely won't happen) the time from initially seeking help for sleep-related issues will go from the supposed "weeks" (because of a perceived lack of ability of the present system to deal with the scope of the problem of OSA, and sleep issues are not just OSA) to "years", or "never". And if these patients pursue problems to to their successful solution, they will need facility-based PSG anyway. So before anybody starts to think that the article about "Diagnosis and Initial Management of Obstructive Sleep Apnea without Polysomnography" is going to solve the world's sleep problems, guess again. BTW, in order to find 81 patients for their study, they had to look at 2216 patients referred to their sleep center (not 2216 people on the street, 2216 people referred to their center, which means they all had a sleep issue) of which 2135 were ineligible for a myriad of reasons.
Heck, if they're gonna cherry-pick like that, even I could have a success rate that good.
That "Sleep Strip" looks better every day, don't it?
SAG

Why that settles it, I'm going to go see my doctor and have him write me a script for that Placebo drug, it must be some kind of a wonder drug, cause I see it used for every disorder you can think of with many times better results.
-
WillSucceed

- Posts: 1031
- Joined: Sun Nov 07, 2004 7:52 am
- Location: Toronto, Ontario
On the contrary, StillAnotherGuest, insomnia is a broad term and cflame1, in her original post, did not use the word. She asked about micro-arousals, getting into stage 4 sleep and, in her last comment, about improving sleep efficiency. It seemed like the thrust of her questions was about getting a better quality of sleep, in particular, reducing micro-arousals and getting Stage 4 sleep, not just getting to sleep.
Overall, insomnia is a term which describes an inability to get to sleep much more so than quality of sleep. Further, it is defined in terms of being transient, acute or chronic and is often, but not always, explainable. Anxiolytics, narcotics, and other sleep-inducers will treat the insomnia, but are no guarantee of a "good" sleep. And while they can treat the insomnia, they certainly are not going to help the person who is having poor sleep because of OSA induced arousals.
So, after having said all that, I think your comment
Overall, insomnia is a term which describes an inability to get to sleep much more so than quality of sleep. Further, it is defined in terms of being transient, acute or chronic and is often, but not always, explainable. Anxiolytics, narcotics, and other sleep-inducers will treat the insomnia, but are no guarantee of a "good" sleep. And while they can treat the insomnia, they certainly are not going to help the person who is having poor sleep because of OSA induced arousals.
So, after having said all that, I think your comment
is of zip help as the term (insomnia) is way too broad. She is having trouble getting QUALITY of sleep, not getting TO sleep.insomnia, whether it's primary or comorbid, has to be considered a core issue here.
Buy a new hat, drink a good wine, treat yourself, and someone you love, to a new bauble, live while you are alive... you never know when the mid-town bus is going to have your name written across its front bumper!
-
StillAnotherGuest

- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Not Done Yet
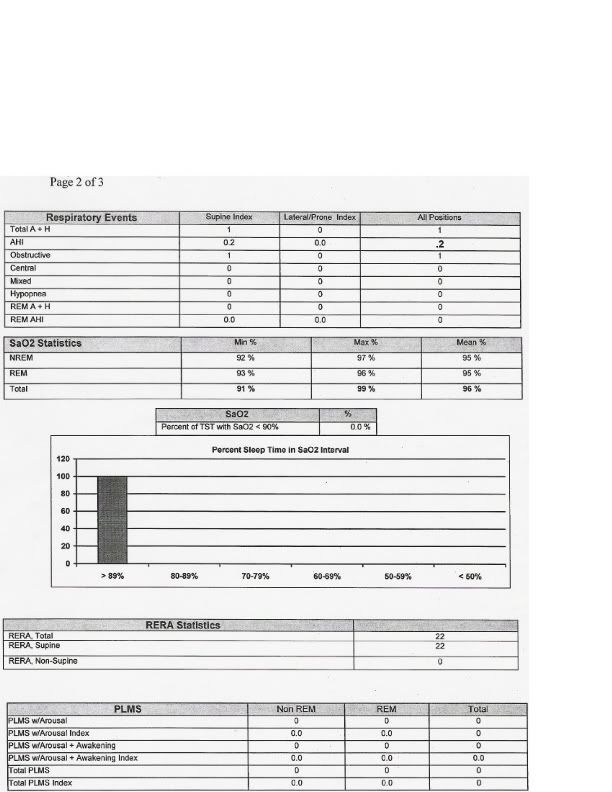
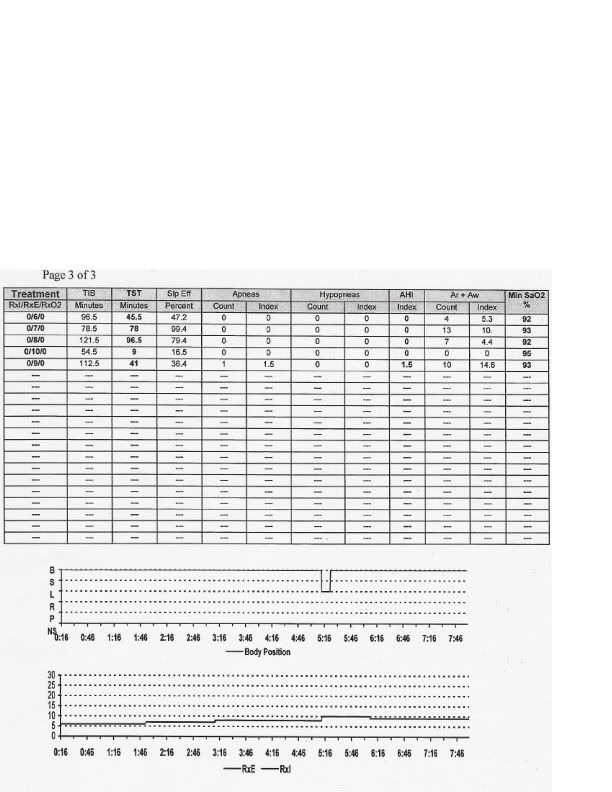
Negative on that, Will. If you can reduce the Arousal Index by 94% to essentially normal levels, and yet the Sleep Efficiency remains abysmal, then there are more issue(s) to resolve. Given the initial commentsWillSucceed wrote:So, after having said all that, I think your commentis of zip help as the term (insomnia) is way too broad. She is having trouble getting QUALITY of sleep, not getting TO sleep.insomnia, whether it's primary or comorbid, has to be considered a core issue here.
it would appear that respiratory issues were addressed.cflame1 wrote:First of all what is a micro arousal? According to what I'm reading I had an index of 112 of these per hour without treatment.. the average over the night went down to an average of 7 over the whole night with treatment.
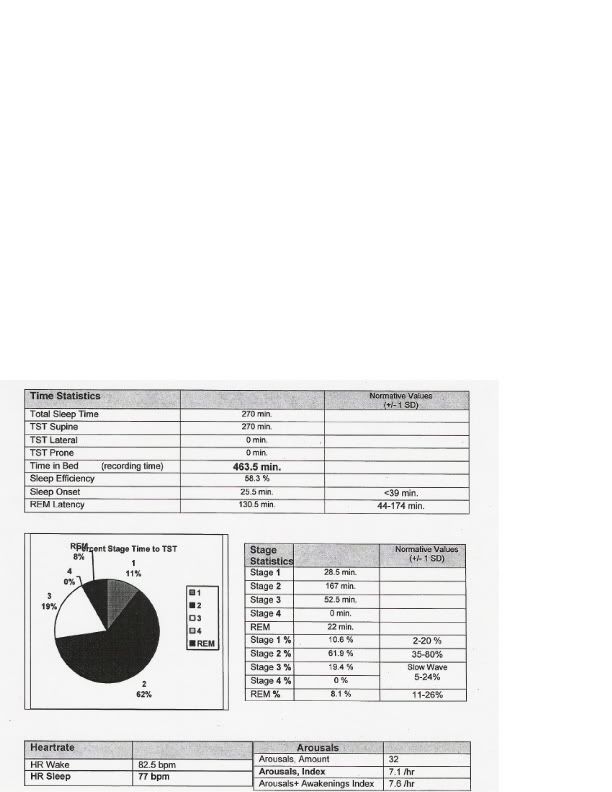
How about improving sleep efficiency? I went from 40% without treatment to 58% with it.
And again, if the problem with Sleep Efficiency is resolved, fine. But abnormal Sleep Efficiency, with or without associated Sleep Fragmentation, cannot be summarily dismissed.
At this point, the term insomnia is being used in a general sense, but no more than "Sleep-Related Breathing Disorder" would be before one differentiates between obstructive, central, UARS, or CSBD. Zeroing in on insomnia characteristics such as co-morbidity, duration, severity and form of presentation will help uncloud the issue.
And if that's not the case with cflame1 (BTW, go Devils!), then perhaps this should at least alert anyone else who may have unresolved or complex sleep issues to continue the search and closely scrutinize all factors that affect sleep.
SAG

Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
SAG,
I've been reading this but not quite following, as some of the terminology is a little over my head. Guess that I should explain that my sleep doc... is a pulmo that also specializes in asthma.
I always thought that insomnia was not sleeping at all. Does it also deal with sleeping for a couple of hours and then waking?
I've been reading this but not quite following, as some of the terminology is a little over my head. Guess that I should explain that my sleep doc... is a pulmo that also specializes in asthma.
I always thought that insomnia was not sleeping at all. Does it also deal with sleeping for a couple of hours and then waking?
-
WillSucceed
- Posts: 1031
- Joined: Sun Nov 07, 2004 7:52 am
- Location: Toronto, Ontario
cflame1 wrote:
Just a thought.
Beautiful! And that, StillAnotherGuest, is the point! You are blathering away about insomnia, comorbidity, , blah, blah, blah... How about saying something helpful, instead of all the "look really clever by baffling them with the blather?"I've been reading this but not quite following, as some of the terminology is a little over my head.
Just a thought.
Buy a new hat, drink a good wine, treat yourself, and someone you love, to a new bauble, live while you are alive... you never know when the mid-town bus is going to have your name written across its front bumper!
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
As We Begin...
The International Classification of Sleep Disorders lists 11 categories of insomnia. However, we're still talking about that general characterization of "difficulty initiating or maintaining sleep or experiencing nonrestorative sleep that results in clinically significant distress or impairment in functioning". These periods of wake can be at the beginning of the night, prior to actual sleep (resulting in a prolonged Sleep Latency), during the middle of the night (reflected in Wake After Sleep Onset) or inappropriate early-morning awakening (which would appear as Wake After Final Arousal).cflame1 wrote:I always thought that insomnia was not sleeping at all. Does it also deal with sleeping for a couple of hours and then waking?
Sleep studies are not used, nor recommended, to assess insomnia. Basically, cause it's only one night. Still, we can get clues from the PSG. Like if sleep efficiency is <85% and wake periods appear where they shouldn't be. Then you take history, and if the patient thinks it's a problem, then it's a problem. You can define it a number of ways. Is there an attributable cause (comorbity) or not (primary), is it acute (days to weeks) or chronic (months to forever) and so on.
But let's table that for a moment. Let me make sure I am clear on one point. You say you are on BiPAP 21/14? I take this from
By your titration results, there were no events on any pressure, so 6 cmH2O took care of everything (OK, maybe a few RERAs in REM, but there no associated desaturations). So 21/14 is pretty aggressive.Current settings 14/21
I guess the first question would be, if low level straight CPAP appears to be pretty effective, how did you happen through APAP and AutoBiPAP?
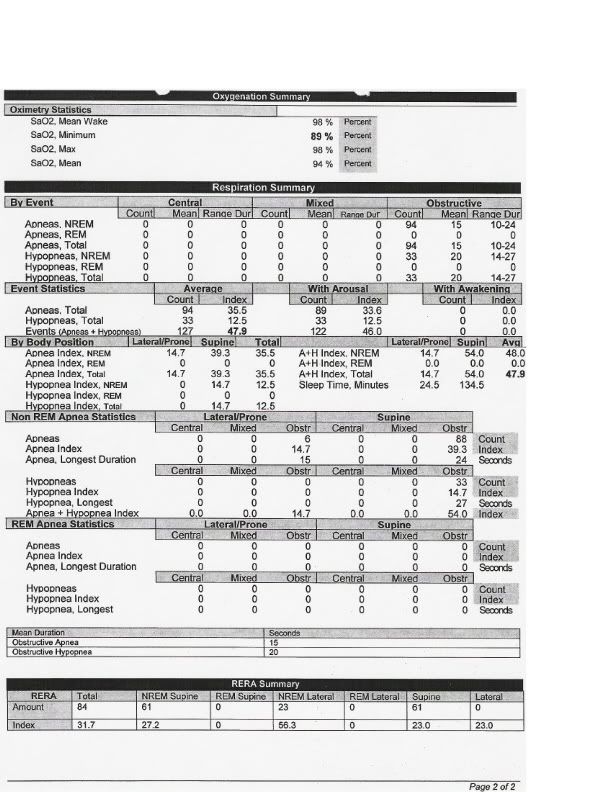
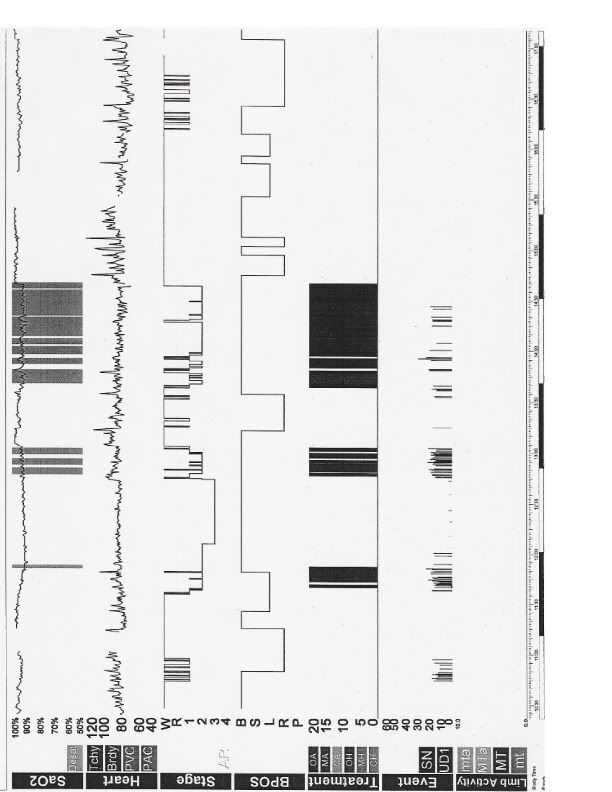
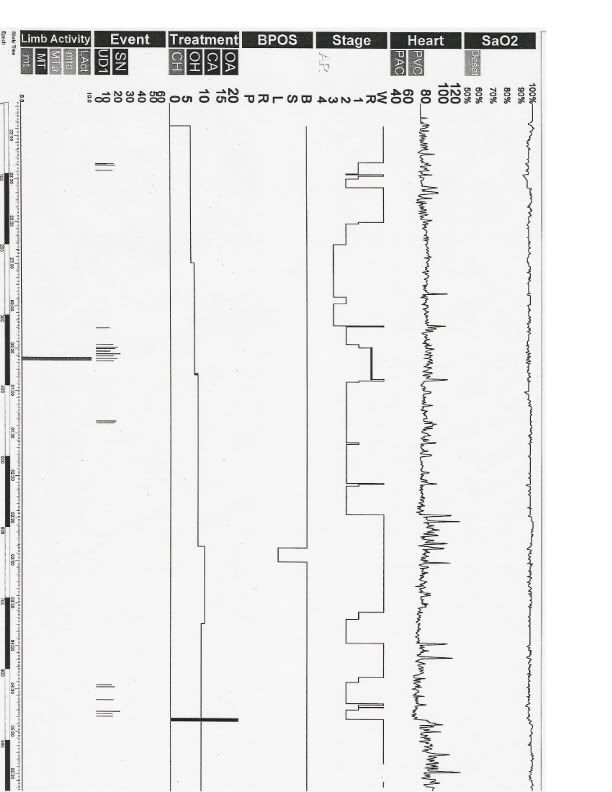
The arousals must be in a light color that they don't seem to show up, but would be nice to get at look at them. The desaturations don't look real impressive, have more of a baseline drop appearance. Gotta keep that asthma thing in mind.
Interesting aside, the lack of REM in diagnostic, reduced and delayed REM in titration, undoubtedly fluoxetine effect.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Someone Else Off The Christmas Card List
On the other hand, we could just go ahead and start to aggravate people. See if you can find out the exact number of desaturations. The scan seems to run the events together, but I'm curious if the number is actually 11, or something significantly greater. And a key point of the study is the area from 1400 to 1430 where there is major event activity. Try to get 5 minute print outs of the epochs (it's not a big deal, there will only be 6 of them, takes 5 minutes tops)(hey, could be worse, we could ask for the 60 30-second epochs, too). This will allow close scrutiny to see if these are bona fide events. I would really like to confirm that they are truly obstructive apneas, and not a product of the automatic scoring button.
SAG
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
SAG,
First of all... my dad has sleep apnea. So there is a family history. He would stop breathing in the hospital multiple times a night and freak out the nurses.
Second of all, I don't think that in this case the fluoxetine is causing the sleep problems (I could be wrong though). I'm sleeping better with it than I did without it, and my days are a lot calmer. My very first study (I don't have the fancy graphs and numbers on that one), had no fluoxetine and they still put me on a xpap.
The Auto to Auto Bipap was my choice. I purchased the Auto Bipap out of pocket.
The 14 EPAP min is what it's taking to keep me asleep at the current time. When it was lower, I would inevitably wake multiple times a night.
First of all... my dad has sleep apnea. So there is a family history. He would stop breathing in the hospital multiple times a night and freak out the nurses.
Second of all, I don't think that in this case the fluoxetine is causing the sleep problems (I could be wrong though). I'm sleeping better with it than I did without it, and my days are a lot calmer. My very first study (I don't have the fancy graphs and numbers on that one), had no fluoxetine and they still put me on a xpap.
The Auto to Auto Bipap was my choice. I purchased the Auto Bipap out of pocket.
The 14 EPAP min is what it's taking to keep me asleep at the current time. When it was lower, I would inevitably wake multiple times a night.
-
WillSucceed
- Posts: 1031
- Joined: Sun Nov 07, 2004 7:52 am
- Location: Toronto, Ontario
cflame1 wrote:
This would suggest that the Prozac is doing it's job in that you are feeling better & enjoying a "calmer" day. However, it easily (and likely) could be impacting your ability to get into Stage 4 sleep. You just are not aware of it and, without the data from the sleep study, would not likely have known.Second of all, I don't think that in this case the fluoxetine is causing the sleep problems (I could be wrong though). I'm sleeping better with it than I did without it, and my days are a lot calmer.
Buy a new hat, drink a good wine, treat yourself, and someone you love, to a new bauble, live while you are alive... you never know when the mid-town bus is going to have your name written across its front bumper!

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
I have been on and off Prozac for years and about 9 months ago took myself off it cold turkey and have not taken it since.
I have read all the pro's and con's of this drug but did not let it influence my taking it or not. I went by how I felt. Even though I deal with depression more now, I feel "better" in other ways if that makes any sense at all. I just didn't like how it made me feel. (A discussion for another time).
Some people need Prozac and that is nothing bad. But others who take it, like myself, can likely get by w/o it and should talk to their doctor about it (which is what you need to do with your concerns). Unfortunately, the med/sleep thing I know nothing about.
I pray I will be able to get by without Prozac for the duration of my life but wouldn't hesitate to take it again if need be. We all have different problems and the ability to cope with them varies. Taking an antidepressant is nothing bad although some who don't know what you are experiencing will try and tell you it is.
Good luck and my prayers will be with you for an overall solution!!
Louise
I have read all the pro's and con's of this drug but did not let it influence my taking it or not. I went by how I felt. Even though I deal with depression more now, I feel "better" in other ways if that makes any sense at all. I just didn't like how it made me feel. (A discussion for another time).
Some people need Prozac and that is nothing bad. But others who take it, like myself, can likely get by w/o it and should talk to their doctor about it (which is what you need to do with your concerns). Unfortunately, the med/sleep thing I know nothing about.
I pray I will be able to get by without Prozac for the duration of my life but wouldn't hesitate to take it again if need be. We all have different problems and the ability to cope with them varies. Taking an antidepressant is nothing bad although some who don't know what you are experiencing will try and tell you it is.
Good luck and my prayers will be with you for an overall solution!!
Louise
_________________
| Mask | |
 |
CPAP Therapy begun 2/6/07
Operating Pressure 10 cm H20
"Any day above ground is a good one."
"Follow your CPAP treatment or you might wake up dead."
Operating Pressure 10 cm H20
"Any day above ground is a good one."
"Follow your CPAP treatment or you might wake up dead."