






SAG,
I'll check with the sleep doc's office and see if I can get them.
Opinion please - questions
-
StillAnotherGuest

- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
The More The Merrier!
Any chance of getting those graphs too? That would really allow a good comparison, and also see how REM behaves (there should be a bunch more without the fluoxetine). Say, how many total studies have you had, anyway?cflame1 wrote:My very first study (I don't have the fancy graphs and numbers on that one), had no fluoxetine and they still put me on a xpap.
And boy, that 21/14 BiPAP sure seems like overkill given the study results. But I guess if you're doing well...
,,,but speaking of which, where do you think you are now, and/or what (if anything) are you looking to change? Are you sleeping through the night or not, and/or still tired/fatigued during the day? Again, if those sleep issues represented in the studies have resolved, then it don't make much sense to pull the bottom can out of the bean display.
SAG

Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
SAG,
Highly unlikely that I'll be able to get anything more from the first study... have their report that they sent to my GP... but she didn't have anything else. Plus it was almost a year ago now. Dunno if they keep stuff that long, seeing as I've never heard from them since the study.
Total... two studies over the course of the past year. One (the first) was a true split night, the second was a two night. I had asthma problems with them all.
I'm sleeping all night, but I'm still tired during the day, especially in the morning. So, needless to say I'd really like to be awake during work hours.
Highly unlikely that I'll be able to get anything more from the first study... have their report that they sent to my GP... but she didn't have anything else. Plus it was almost a year ago now. Dunno if they keep stuff that long, seeing as I've never heard from them since the study.
Total... two studies over the course of the past year. One (the first) was a true split night, the second was a two night. I had asthma problems with them all.
I'm sleeping all night, but I'm still tired during the day, especially in the morning. So, needless to say I'd really like to be awake during work hours.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Moving Along...
OK, get that test report from the first (split) study, it should still offer some information.
I think until proven otherwise, we'll have to consider that the sleep architecture seen in the 2 studies you've presented so far is fairly representative as to how you normally sleep. As such, your slow wave sleep, at 24.2% in the first study and 19.4% in the second, is fine, as is it's location (first sleep cycle) and stability (event-free, but eventually we have to see all the arousal ticks, although I'm pretty sure there won't be any). If we believe that your total sleep quantity is down, which is where we're at now, SWS% may drop a little, relatively speaking, but it should still be OK. BTW, there is no clinical difference between Stage 3 and Stage 4 SWS, (unless you're about 10, you don't don't see too much Stage 4). When the new scoring parameters come out in a couple months, the Stage 3 and 4 differentiation should change.
Ooh, almost forgot re: quality of SWS - ask them if there was any alpha intrusion there. If they go "Hah?" then hit 'em upside the head with a torque wrench. If you don't have a torque wrench, borrow RG's.
Despite all the asthma concerns, I see you never mention medications for that. Are you on any regularly, or on an as-needed basis?
Were you ever asked about strange sensations (visual or auditory hallucinations) immediately before sleep or immediately after awakening? Or sudden weakness after strong emotion (laughter, etc.)? Ever had a severe head injury, especially one that resulted in loss of consciousness, however long?
I'm thinking another field trip to the sleep lab is in the works. It may take the form of (1) full night diagnostic (no CPAP) to confirm the presence/extent of sleep-disordered breathing. The asthma must be tuned-up prior to this; (2) full night titration on ideal pressure (and I really don't see how that could be BiPAP 21/14); (3) full night study, with or without CPAP (won't matter which, as long as you're stable), followed by a daytime nap study, called MSLT (multiple sleep latency test), to objectively quantify daytime sleepiness and look for REM. This option would undoubtedly require discontinuing the fluoxetine for a couple weeks to remove it's influence on sleep disruption and/or REM; and/or (4) an all-out attack on the possibility of insomnia, including accurate differentiation and treatment regimen (a major part of which would be the use Cognitive Behavioral Therapy (CBT)).
Regardless, we're gonna need a top-flight sleep specialist here shortly, none of this is really self-help stuff you can do at home (oh Noam? Noam? How come you're not answering, Noam?) Sorry, inside joke.
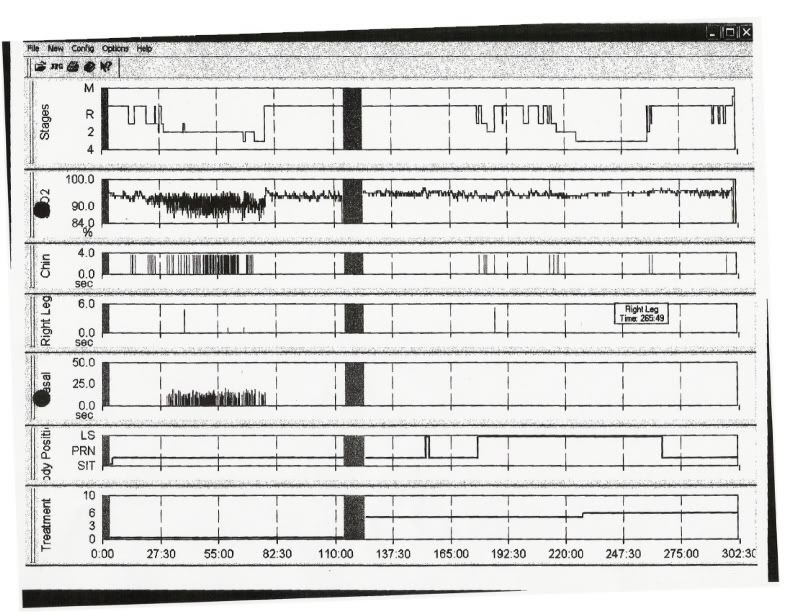
Can you get a copy of the graphs you posted that show the location of the arousals?
Time to get down to the docks, got a big container ship to unload today.
SAG
I think until proven otherwise, we'll have to consider that the sleep architecture seen in the 2 studies you've presented so far is fairly representative as to how you normally sleep. As such, your slow wave sleep, at 24.2% in the first study and 19.4% in the second, is fine, as is it's location (first sleep cycle) and stability (event-free, but eventually we have to see all the arousal ticks, although I'm pretty sure there won't be any). If we believe that your total sleep quantity is down, which is where we're at now, SWS% may drop a little, relatively speaking, but it should still be OK. BTW, there is no clinical difference between Stage 3 and Stage 4 SWS, (unless you're about 10, you don't don't see too much Stage 4). When the new scoring parameters come out in a couple months, the Stage 3 and 4 differentiation should change.
Ooh, almost forgot re: quality of SWS - ask them if there was any alpha intrusion there. If they go "Hah?" then hit 'em upside the head with a torque wrench. If you don't have a torque wrench, borrow RG's.
Despite all the asthma concerns, I see you never mention medications for that. Are you on any regularly, or on an as-needed basis?
Were you ever asked about strange sensations (visual or auditory hallucinations) immediately before sleep or immediately after awakening? Or sudden weakness after strong emotion (laughter, etc.)? Ever had a severe head injury, especially one that resulted in loss of consciousness, however long?
I'm thinking another field trip to the sleep lab is in the works. It may take the form of (1) full night diagnostic (no CPAP) to confirm the presence/extent of sleep-disordered breathing. The asthma must be tuned-up prior to this; (2) full night titration on ideal pressure (and I really don't see how that could be BiPAP 21/14); (3) full night study, with or without CPAP (won't matter which, as long as you're stable), followed by a daytime nap study, called MSLT (multiple sleep latency test), to objectively quantify daytime sleepiness and look for REM. This option would undoubtedly require discontinuing the fluoxetine for a couple weeks to remove it's influence on sleep disruption and/or REM; and/or (4) an all-out attack on the possibility of insomnia, including accurate differentiation and treatment regimen (a major part of which would be the use Cognitive Behavioral Therapy (CBT)).
Regardless, we're gonna need a top-flight sleep specialist here shortly, none of this is really self-help stuff you can do at home (oh Noam? Noam? How come you're not answering, Noam?) Sorry, inside joke.
Can you get a copy of the graphs you posted that show the location of the arousals?
Time to get down to the docks, got a big container ship to unload today.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
Asthma stuff... it's as needed and it's ventolin. I've been on it for years, though I rarely need it. Tried taking it prior to masking up, but then I'd sit and feel my heart race. Not an easy thing to try and sleep with.
I was asked about the sensations and the weakness... and the answer to that is no. Head injury? Closest to that was a car wreck when I was in about grade 3 (I think). Two black eyes, and they thought that I had a concussion.
I'll have to make some calls, which from the looks of the weather today could be a fun endeavor (not). Probably a bunch of people out today with the blizzard coming.
I was asked about the sensations and the weakness... and the answer to that is no. Head injury? Closest to that was a car wreck when I was in about grade 3 (I think). Two black eyes, and they thought that I had a concussion.
I'll have to make some calls, which from the looks of the weather today could be a fun endeavor (not). Probably a bunch of people out today with the blizzard coming.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Time To Get Started...
A bunch of things of interest in this first study.
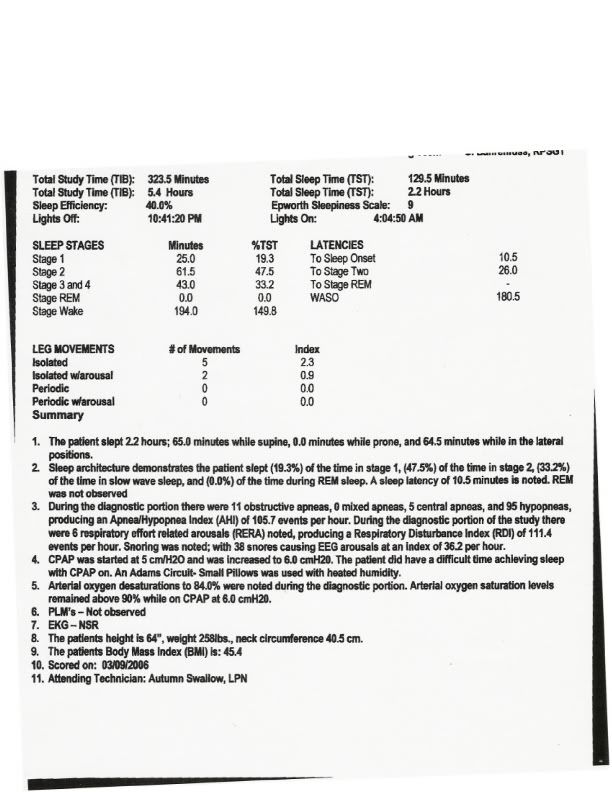
Now, this was without fluoxetine, right? The lack of REM is again noted, but that could be a result of the lack of sufficient continuous sleep (you need about 90 minutes to get a REM period going)(the lack of an early REM removes further consideration of the visual/auditory hallucination thing).
Right, the lack of continuous sleep. Here, the sleep onset latency is good, but overall efficiency is abysmal. If this was the only study, then maybe you could consider CPAP intolerance or lab effect to an extent (yet you are able to achieve sustained SWS after a bit) but with a steady pattern of very poor sleep efficiency for all 3 and continued sleepiness, then insomnia becomes a core issue. Whether fluoxetine makes it worse is now up for debate.
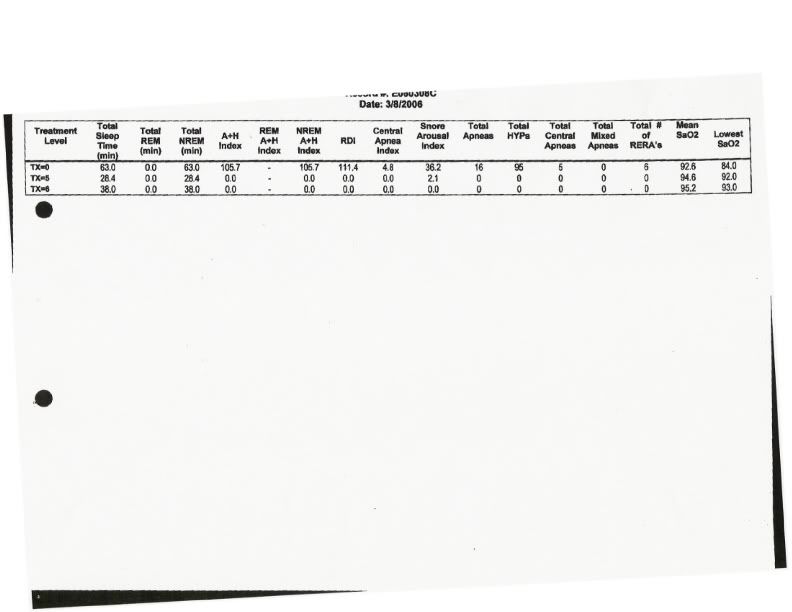
In this study, the respiratory events are remarkable for their significant desaturations. Comparing the two ambient studies, the first shows each respiratory event resulting in a desat of about 6%:

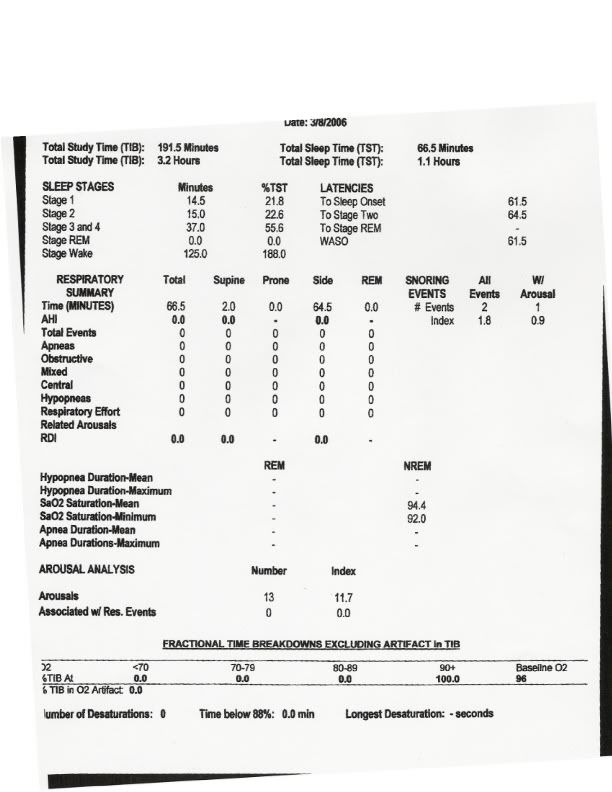
Contrast this with the most recent study, especially the area that we're trying to get printouts for:

and you can see how the events have virtually no corresponding desaturation. Did you lose significant weight between the two studies? If so, these results should give great encouragement as to what weight loss could continue to do here.
Again, low-level CPAP is completely effective in addressing respiratory events. That 21/14 BiPAP is like a sledgehammer to kill a mosquito.
So time to start attacking the insomnia. All the rules of basic sleep hygiene need to be followed. The aforementioned Cognitive Behavior Therapy should be of great help. The Board-Certified Sleep Specialist should be able to help with this, but the treatment of insomnia, including the use of CBT, is somewhat of a sub-specialty in Sleep Medicine.
There"s been a lot of stuff out lately about using eszopiclone in combination with fluoxetine to treat depression and insomnia. Fava has done a lot of work in this area, check out the Sepracor list
Eszopiclone/Fluoxetine Co-Therapy
if you want to consider the pharmaceutical route. Of course, long-term use of sleep aids is not recommended. Actually, a lot of people think short-term use of sleep aids is not recommended, but the newer drug classes are sure a heckuva lot better than what used to be out there.
Till the other stuff comes...
SAG
Now, this was without fluoxetine, right? The lack of REM is again noted, but that could be a result of the lack of sufficient continuous sleep (you need about 90 minutes to get a REM period going)(the lack of an early REM removes further consideration of the visual/auditory hallucination thing).
Right, the lack of continuous sleep. Here, the sleep onset latency is good, but overall efficiency is abysmal. If this was the only study, then maybe you could consider CPAP intolerance or lab effect to an extent (yet you are able to achieve sustained SWS after a bit) but with a steady pattern of very poor sleep efficiency for all 3 and continued sleepiness, then insomnia becomes a core issue. Whether fluoxetine makes it worse is now up for debate.
In this study, the respiratory events are remarkable for their significant desaturations. Comparing the two ambient studies, the first shows each respiratory event resulting in a desat of about 6%:
Contrast this with the most recent study, especially the area that we're trying to get printouts for:
and you can see how the events have virtually no corresponding desaturation. Did you lose significant weight between the two studies? If so, these results should give great encouragement as to what weight loss could continue to do here.
Again, low-level CPAP is completely effective in addressing respiratory events. That 21/14 BiPAP is like a sledgehammer to kill a mosquito.
So time to start attacking the insomnia. All the rules of basic sleep hygiene need to be followed. The aforementioned Cognitive Behavior Therapy should be of great help. The Board-Certified Sleep Specialist should be able to help with this, but the treatment of insomnia, including the use of CBT, is somewhat of a sub-specialty in Sleep Medicine.
There"s been a lot of stuff out lately about using eszopiclone in combination with fluoxetine to treat depression and insomnia. Fava has done a lot of work in this area, check out the Sepracor list
Eszopiclone/Fluoxetine Co-Therapy
if you want to consider the pharmaceutical route. Of course, long-term use of sleep aids is not recommended. Actually, a lot of people think short-term use of sleep aids is not recommended, but the newer drug classes are sure a heckuva lot better than what used to be out there.
Till the other stuff comes...
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Let's See If We Can Fill A Whole Page
OK, great, maybe we're leaning a little more towards primary insomnia, but we got a ways to go yet.
If you're waiting around in the doctor's office looking for something to read and all you can find is a 1997 Sports Illustrated, try this. It's a great handbook by The Lung Association of Canada that covers a wide range of topics not only about sleep apnea itself but about a lot of other inter-related factors, including sleep hygiene.
Sleep Apnea Action Handbook
You can dig a little deeper into sleep hygiene than the Canada Handbook offers, here's pointers from WebMD that offer a good summary:
In re: the Ventolin, there's 2 general concepts to the treatment of asthma, control and rescue. Ventolin is a rescue inhaler. Perhaps that whole approach needs a going over, too. You don't by any chance have a "peak flow meter" lying around, do you? If so, ever do any early morning (and I mean like 4:00 AM) measurements?
Oh God, cruise ship coming in today, I hate tourists with giant bags of grapefruit that they're never going to eat anyway.
SAG
If you're waiting around in the doctor's office looking for something to read and all you can find is a 1997 Sports Illustrated, try this. It's a great handbook by The Lung Association of Canada that covers a wide range of topics not only about sleep apnea itself but about a lot of other inter-related factors, including sleep hygiene.
Sleep Apnea Action Handbook
You can dig a little deeper into sleep hygiene than the Canada Handbook offers, here's pointers from WebMD that offer a good summary:
Special attention should be made to the line about "Reducing sleep by as little as one and a half hours for just one night reduces daytime alertness by about one-third." You need about 7.5 hours of total sleep per night (450 minutes). With your sleep studies showing sleep times of 128.5, 159 and 270 minutes, unless your sleep quality is dramatically better, you're in a hole that's getting deeper. (Hmmm, need a post going over the concept of "Sleep Debt." We'll have to work that in somehow.)How to Sleep Better
'Sleep Hygiene' Solutions for Better Sleep By Michael J. Breus, ABSM, PhD; WebMD FeatureReviewed by Charlotte Grayson Mathis, MD
From having occasional difficulty sleeping to insomnia, there is a lot you can do to get a better night's sleep, feel refreshed when you awake, and remain alert throughout the day. It's called "sleep hygiene" and refers to those practices, habits, and environmental factors that are critically important for sound sleep. And most of it is under your control.
There are four general areas important to sleep hygiene:
Our circadian rhythm, or 24-hour cycle
Aging
Psychological stressors -- those factors can cause difficulty falling asleep and disturb the quality of your sleep
Common social or recreational drugs like nicotine, caffeine, and alcohol
Circadian Rhythm
We all have a day-night cycle of about 24 hours called the circadian rhythm. It greatly influences when we sleep and the quantity and the quality of our sleep. The more stable and consistent our circadian rhythm is, the better our sleep. This cycle may be altered by the timing of various factors, including naps, bedtime, exercise, and especially exposure to light (from traveling across time zones to staring at that laptop in bed at night).
Aging
Aging also plays a role in sleep and sleep hygiene. After the age of 40 our sleep patterns change, and we have many more nocturnal awakenings than in our younger years. These awakenings not only directly affect the quality of our sleep, but they also interact with any other condition that may cause arousals or awakenings, like the withdrawal syndrome that occurs after drinking alcohol close to bedtime. The more awakenings we have at night, the more likely we will awaken feeling unrefreshed and unrestored.
Psychological Stressors
Psychological stressors like deadlines, exams, marital conflict, and job crises may prevent us from falling asleep or wake us from sleep throughout the night. It takes time to "turn off" all the noise from the day. No way around it. If you work right up to the time you turn out the lights, or are reviewing all the day's events and planning tomorrow (sound familiar?), you simply cannot just "flip a switch" and drop off to a blissful night's sleep.
One must develop some kind of pre-sleep ritual to break the connection between all the stress and bedtime. This is perhaps even more important for children. These rituals can be as short as 10 minutes or as long as an hour. Some find relief in making a list of all the stressors of the day, along with a plan to deal with them, as it serves to end the day. Combining this with a period of relaxation, perhaps by reading something light, meditating, or taking a hot bath can also help you get better sleep. And don't look at that clock! That tick-tock will tick you off.
Social or Recreational Drugs
Social or recreational drugs like caffeine, nicotine, and alcohol may have a larger impact on your sleep than you realize. Caffeine, which can stay in your system as long as 14 hours, increases the number of times you awaken at night and decreases the total amount of sleep time. This may subsequently affect daytime anxiety and performance. The effects of nicotine are similar to those of caffeine, with a difference being that at low doses, nicotine tends to act as a sedative, while at high doses it causes arousals during sleep.
Alcohol may initially sedate you, making it easier to fall asleep; however, as it is metabolized and cleared from your system during sleep, it causes arousals that can last as long as two to three hours after it has been eliminated. These arousals disturb sleep, often causing intense dreaming, sweating, and headache. Smoking while drinking caffeine and alcohol can interact to affect your sleep dramatically. These sleep disturbances may be most apparent upon awakening, feeling unrefreshed, groggy, or hungover.
It is important to realize that not getting the proper amount of and the best quality sleep may have serious short-term and long-term consequences. Many studies have shown that sleep deprivation adversely affects performance and alertness.
Reducing sleep by as little as one and a half hours for just one night reduces daytime alertness by about one-third. Excessive daytime sleepiness impairs memory and the ability to think and process information, and carries a substantially increased risk of sustaining an occupational injury. Long-term sleep deprivation from sleep disorders like apnea have recently been implicated in high blood pressure, heart attack, and stroke.
All that said, here are some sleep hygiene tips to help you relax, fall asleep, stay asleep, and get better sleep so that you wake up refreshed and alert.
1. Avoid watching TV, eating, and discussing emotional issues in bed. The bed should be used for sleep and sex only. If not, we can associate the bed with other activities and it often becomes difficult to fall asleep.
2. Minimize noise, light, and temperature extremes during sleep with ear plugs, window blinds, or an electric blanket or air conditioner. Even the slightest nighttime noises or luminescent lights can disrupt the quality of your sleep. Try to keep your bedroom at a comfortable temperature -- not too hot (above 75 degrees) or too cold (below 54 degrees).
3. Try not to drink fluids after 8 p.m. This may reduce awakenings due to urination.
4. Avoid naps, but if you do nap, make it no more than about 25 minutes about eight hours after you awake. But if you have problems falling asleep, then no naps for you.
5. Do not expose your self to bright light if you need to get up at night. Use a small night-light instead.
6. Nicotine is a stimulant and should be avoided particularly near bedtime and upon night awakenings. Having a smoke before bed, although it may feel relaxing, is actually putting a stimulant into your bloodstream.
7. Caffeine is also a stimulant and is present in coffee (100-200 mg), soda (50-75 mg), tea (50-75 mg), and various over-the-counter medications. Caffeine should be discontinued at least four to six hours before bedtime. If you consume large amounts of caffeine and you cut your self off too quickly, beware; you may get headaches that could keep you awake.
8. Although alcohol is a depressant and may help you fall asleep, the subsequent metabolism that clears it from your body when you are sleeping causes a withdrawal syndrome. This withdrawal causes awakenings and is often associated with nightmares and sweats.
9. A light snack may be sleep-inducing, but a heavy meal too close to bedtime interferes with sleep. Stay away from protein and stick to carbohydrates or dairy products. Milk contains the amino acid L-tryptophan, which has been shown in research to help people go to sleep. So milk and cookies or crackers (without chocolate) may be useful and taste good as well.
10. Do not exercise vigorously just before bed, if you are the type of person who is aroused by exercise. If this is the case, it may be best to exercise in the morning or afternoon (preferably an aerobic workout, like running or walking).
11. Does your pet sleep with you? This, too, may cause arousals from either allergies or their movements in the bed. Thus, Fido and Kitty may be better off on the floor than on your sheets.
Good sleep hygiene can have a tremendous impact upon getting better sleep. You should wake-up feeling refreshed and alert, and you should generally not feel sleepy during the day. If this is not the case, poor sleep hygiene may be the culprit, but it is very important to consider that you may have an unrecognized sleep disorder. Many, many sleep disorders go unrecognized for years, leading to unnecessary suffering, poor quality of life, accidents, and great expense. Since it is clear how critical sound sleep is to your health and well-being, if you are not sleeping well, see your doctor or a sleep specialist.
In re: the Ventolin, there's 2 general concepts to the treatment of asthma, control and rescue. Ventolin is a rescue inhaler. Perhaps that whole approach needs a going over, too. You don't by any chance have a "peak flow meter" lying around, do you? If so, ever do any early morning (and I mean like 4:00 AM) measurements?
Oh God, cruise ship coming in today, I hate tourists with giant bags of grapefruit that they're never going to eat anyway.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
You Have To Pick Something
Who prescribed the fluoxetine in the first place? That you mention stress vs depression as the reason for taking fluoxetine makes one suddenly take pause. If the flow is depression > anxiety > insomnia then maybe the SSRI approach might be appropriate, but if it's anxiety > insomnia then you might want to reconsider. I would grab the Board-Certified Sleep Specialist by the scruff and get a definitive ruling on that.cflame1 wrote: I wouldn't be surprised that in my case it would be psychological stress...It would be the reason that I ended up on the fluoxetine in the first place.
Y'know, it's about time to get a Team Leader to assess the risk/benefits of all this stuff. You have asthma that prevents you from sleeping. You have an inhaler for the asthma that you can't take because it prevents you from sleeping. You're taking an SSRI that undoubtedly is disrupting your sleep. And a 21/14 BiPAP pressure that is based on... what is it based on again?
I think it's just about time to erase the blackboard and start from scratch.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
SAG,
Well they got a little confused with what I was asking them for. I have an appointment to see the sleep doc on the 24th, with them trying to get me in sooner. I'll talk to him about my meds... see if they need to be changed.
The tech jumped a little when I told her about a conversation that I'd had with my mother the other night. Turns out that my mother has narcolepsy, and has for awhile. Not sure if that will make any difference or not.
Well they got a little confused with what I was asking them for. I have an appointment to see the sleep doc on the 24th, with them trying to get me in sooner. I'll talk to him about my meds... see if they need to be changed.
The tech jumped a little when I told her about a conversation that I'd had with my mother the other night. Turns out that my mother has narcolepsy, and has for awhile. Not sure if that will make any difference or not.
I guess that I did make them jump. The sleep doc called me tonight and wants to set up a PSG/MSLT... with me off the fluoxetine.
Going to see if I can get to sleep tonight without it. The study's in 10 days.
Said that there is a possibility that it could be one of a couple of things (in conjunction with the OSA), not the least of which is narcolepsy.
Going to see if I can get to sleep tonight without it. The study's in 10 days.
Said that there is a possibility that it could be one of a couple of things (in conjunction with the OSA), not the least of which is narcolepsy.
-
sleepyjane
- Posts: 176
- Joined: Tue Feb 27, 2007 1:43 am