FrederickRose wrote: Are there situations where it takes one minimum pressure to treat OSA other than REM-OSA and a significantly higher minimum pressure to treat OSA including REM-OSA? And if so, which is the better scenario?
Gosh yes, I have it myself and I will see if I can dig out some report examples to show you.
I did have an in lab diagnsotic sleep study and titration.
My AHI overall was 12 but in REM 53 and I had desats to very low 70s.
I sometimes need 6 to 8 cm more pressure in what appears to be REM (after 8 years I have learned to spot the probable REM times quite easily).
I came out of the titration sleep study with a RX of 8. But it was the titration study from hell and I slept poorly and only got 6 minutes of REM sleep.
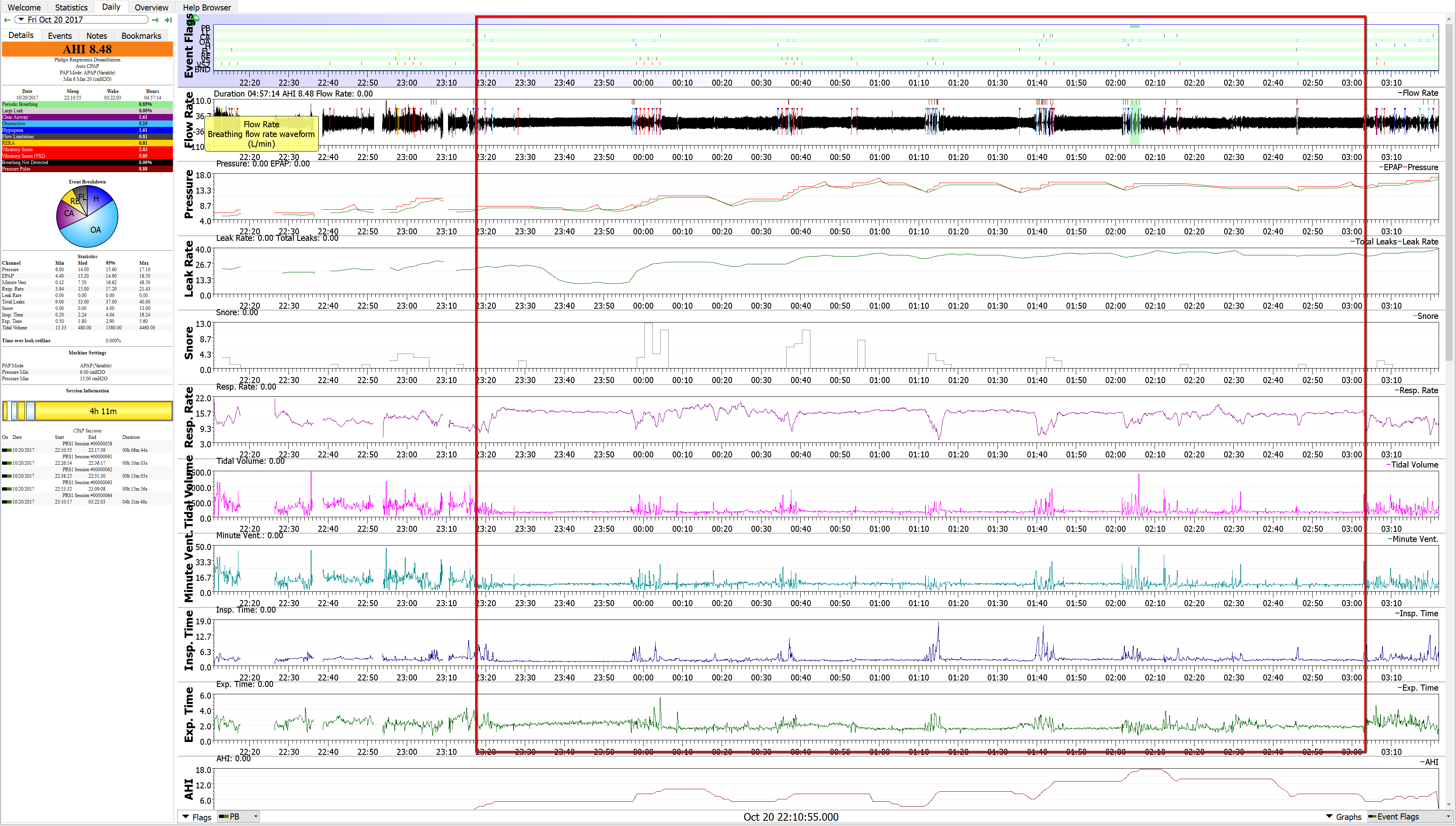
Using my Respironics APAP I self titrated at home and found I was needing 16 to 18 cm at times during probable REM.
With 8 cm minimum it couldn't get to 18 quick enough and couldn't hold the airway open well enough to prevent the collapse in the first place...my AHI numbers were running 8 to 10 to 12. Once I increased to 10 minimum (I went up in 0.5 cm increments) the AHI was cut down to 2 to 4. Acceptable numbers and I left it that way for about 6 weeks with no other changes and it dropped to the 1 to 2 range.
REM worse OSA is very common...and I am a prime example of it.
And yes...it needs to be treated....desats can be brutal even in just REM. I was having massive headaches every morning from the desat imbalance of gases.
Let me go see if I can find an old example to how you. It's been 8 years and the place where I have my old reports is now on my shit list because they want me to pay $400 a year to do what they used to let me do free.
I do wish you had got a ResMed AirSense 10 AutoSet though. Will explain about that in more detail later once you get your minimum worked up to around 9 or 10 and we see the results.
I may have to RISE but I refuse to SHINE.