rkl122 wrote: because the more I study the flow trace at strong zoom level, the more scared I get
Ron... Chill!
There's nothing to be scared about. You're letting your inquiring mind and imagination run away with you.
You have poor sleep. Lot's of causes for that. Sleep Disordered Breathing is one, caffeine is another, I'm just sayin'. Obsessing over it is a major cause - again, just sayin'.
Yes, I like average better than median most of the time. Statisticians like median, I guess, because it is not affected so much by any large outliers in the sample. On the hand, the median doesn't work well if there is a large spread in the data. Take my leaks for example, the median is most often is Zero, which doesn't tell me much, while the average might be a low number which I can compare with another night's. I like graphic presentations best where I can see what's happening.
Anyway, back to you. You have some Flow Waves that are not "typical". So, we need to investigate why that might be. The first thing is that disturbed sleep from any cause and being awake will produce waveforms that are not typical. The second thing is that we are working with inadequate and incomplete sensing capability with marginal analyzing ability. When we see something in our data, sometimes the best we can do is say, "Oh, that looks, like it might be this". The this being something that came from a lab with a full array of sensors, analytical computers, and experts who have studied the subject for years.
Sleep Labs will likely have at least 12 channels of information to analyze. We have 1, maybe 3, if we have a pulse-Ox.
Our one sensor is a flow rate detector - in the machine! It's not even close to our respiratory tract. The lab will use sensors at the nose and mouth to determine nasal and oral flow. We have no way to directly determine either. If we are using a nasal mask, any mouth expiratory flow is not detected and is assumed to be a leak equal to the sum of the inspiratory flow minus any expiratory nasal flow that is detected during that cycle. Inspiratory flow is assumed to be the change in outflow from the machine over static leak. With a nasal mask, any oral inflow is not detected. With a nasal mask, any oral inflow (mouth breathing) is not detected, not detected, and will be seen as a flat line on the flow rate graphic. Yeah, I said it twice. (modern machines use algorithms and high powered mathematics to overcome these shortcomings, but still there is only one remotely located sensor)
So right away, at home, particularly if using a nasal mask, we've taken away the ability to directly measure and perhaps accurate depict the Flow Rate Wave - The only thing, really, being sensed. So, we have to be careful when we say, "this looks like that."
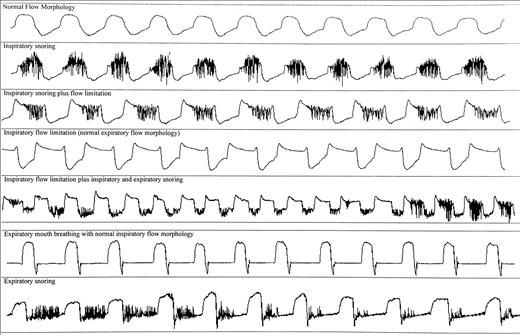
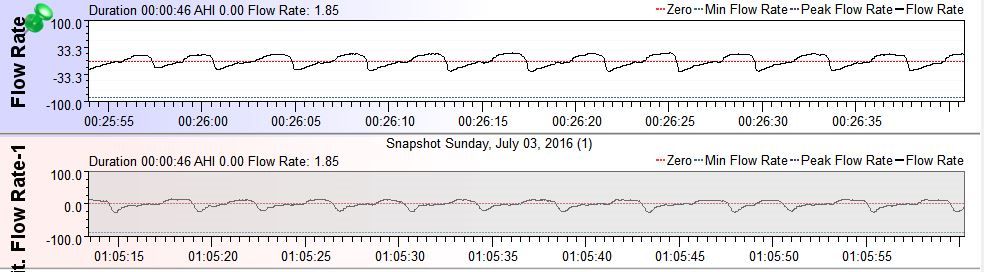
Some of your breathing
looks like it could include some mouth breathing. The top (early) example is relatively normal, the second (later) example has the characteristically flatter expiratory curve of exhaling through the mouth.
Have a look at the expiratory mouth breathing example in the graphic immediately below. This graphic is important because it uses a only a nasal sensor so the waves are going to be similar to those using a nasal mask. Also, review that other
link I sent which uses the other graphic below to explain the effects of mouth breathing on flow. Also, consider the algorithms your machine uses to apply EPAP and IPAP (I don't have a clue and I don't feel like researching it) All of these things will have an influence on the shape of the flow wave graphic.
One thing that you might want to consider - using a FFM with a fixed pressure. That would eliminate some of the unknowns for analytical purposes.
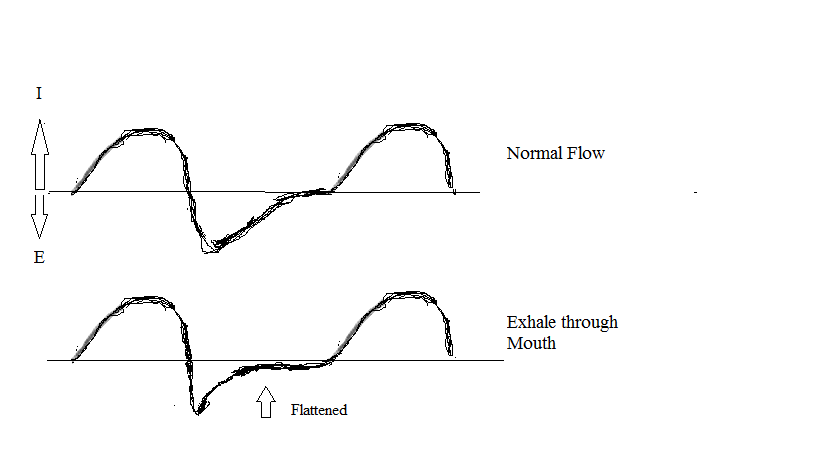
 Below: How the shape tends to change with an increase in mouth expiration
Below: How the shape tends to change with an increase in mouth expiration
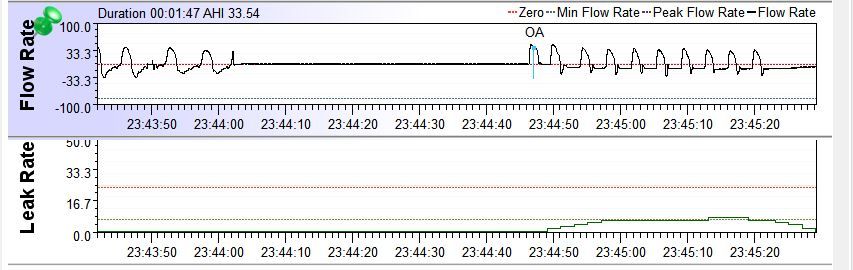
And More: Notice at the top right, total exhalation by mouth, the relatively small leak detected. Only about 8
Jay Aitchsee wrote:Flow wave examples of mouth breathing wearing a nasal mask:
23:44:00 to 23:44:44 Total mouth breathing on inhale and exhale, 44 second apnea scored at resumption of nasal breathing, no leaks scored.
23:44:50 to 23:45:20 Nasal inhalation with exhalation totally by mouth scored as leak.
---------------------------------------------------------------------------
Below:
Normal sleep breathing on top, expiratory mouth breathing on the bottom in large leak (shaded area)
Notice the flattening of the expiratory portion of the wave with exhalation by mouth.
Edit: Times corrected








