







Guest,
I think your choice of a RemStar AUTO (w/Cflex?) is an EXCELLENT choice! The issue of whether an APAP can or cannot preempt all apnea events remains fodder for debate, there is truth on both sides of the discussion. I would complicate the discussion even further by distinguishing between "technical" apnea events (they meet certain objective criteria), and "clinically significant" apnea events. During my sleep study the average apnea duration was on the order of a minute. Since I started using the RemStar AUTO, the data records an average duration of 12 seconds. I would venture that almost anybody could hold their breath that long and hardly notice it. And as has been suggested, if you MUST have CPAP, an APAP will morph back and forth easily. Even if you only planned to use it in CPAP mode, it might still be worth the difference to occasionally flip it into APAP mode and do another in-home sleep study (without the hassle and expense of "begging" your doctor and your insurance). I prefer leaving it in AUTO mode all the time, makes for an easier breathing experience, and I also get a continuous-running sleep study which has been VERY enlightening.
APAP Does Not Work As Good as BiPap?
-
Guest
I understand an APAP can be used as a CPAP too, but I'm leary now that I've learned an APAP can't do what I thought it could do. If I'm going to use it as CPAP, why spend the money for an APAP? This has been a big eye-opener for me. I have seen a lot of posts about how the range set on an APAP is important and it's my understanding I'd learn what to set it to by looking at the software data, but if I do decide to spring for an APAP and set the low end to my current pressure and the top end 3 or 4 more than that, but it can't change pressure rapidly enough to preempt apneas, what good is it?NightHawkeye wrote:Since you asked for my recommendation, I'd still recommend an APAP, although I suspect that the minimum pressure needs to be set close to the 90% pressure to eliminate the sort of residual apneas which show up in my own data, and then open the APAP maximum pressure up a little above that. An APAP gives you more options, just be sure to keep realistic expectations.
Bill has unequivocal data that the Respironics auto can't change pressure rapidly enough to preempt apneas. That's not something you can debate. For me this has been very important news and I think everyone should be made aware that an APAP can't preempt apneas because for me anyway, that's the main reason I was considering it. I thought it could reach up and get what a regular CPAP couldn't. I'm glad I found this topic before I ordered. Everyone has been so helpful and informative and I've learned so much more than I knew before. Especially about APAPs and how they work and what they can and can't do.Ric wrote:The issue of whether an APAP can or cannot preempt all apnea events remains fodder for debate, there is truth on both sides of the discussion.
But I do like the idea of using an APAP in lieu of a sleep study as Ric suggested. That makes good sense. Now I have to reconsider again. This isn't an easy one to decide.

Anonymous wrote:Since I was about to order the Remstar APAP, that's not what I wanted to hear. Would this be true for everyone using the Respironics APAP? That it can't work fast enough to preempt apneas? If your beginning pressure is high enough so it doesn't have so far to go up to preempt apneas does it still not work right?NightHawkeye wrote:I've already reached my conclusion regarding APAP's, and my conclusion is that the Respironics APAP algorithm cannot change pressure rapidly enough to pre-empt apneas. The data is unequivocal.
I've been doing a lot of research and was about to upgrade from my Fisher & Paykel and order the Respironics APAP mostly because of the overwhelmingly good reviews on this board, but this fact changes everything. If it can't preempt apneas, why spend the extra money?
Can the Resmed APAP change pressure rapidly enough to preempt apneas? Or should I steer clear of all APAPs and stick with a regular CPAP machine? Which one would you recommend?
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
>>
I understand an APAP can be used as a CPAP too, but I'm leary now that I've learned an APAP can't do what I thought it could do. If I'm going to use it as CPAP, why spend the money for an APAP? This has been a big eye-opener for me. I have seen a lot of posts about how the range set on an APAP is important and it's my understanding I'd learn what to set it to by looking at the software data, but if I do decide to spring for an APAP and set the low end to my current pressure and the top end 3 or 4 more than that, but it can't change pressure rapidly enough to preempt apneas, what good is it?
<<
Hi,
I think this is a misinterpretation of the discussions thus far.
AUTOs *do* pre-empt apneas. All we have been discussing in detail is how an auto might handle 'sudden' apneas (the hypothetical case mentioned) & thus far the information provided here can be taken to show that depending on exactly the circumstances, the Auto may be close enough in required pressure to make a difference or it may be succesful in preventing the next one.
The bottom line in deciding if an AUTO is good for you is how well they work for others and I think there is enough feedback here to show a lot of happy users.
One great incentive to buy an AUTO was that they provided vastly superior data to what most cpap machines did. That is changing slowly but still applies today.
>>
But I do like the idea of using an APAP in lieu of a sleep study as Ric suggested. That makes good sense. Now I have to reconsider again. This isn't an easy one to decide.
<<
Yes, this is the value proposition that AUTOs bring to the table. They can function as both AUTO and CPAP - because of this they can be used to reasses ones 90% pressure requirement whenever the user wants & if running in pure AUTO mode is not achieving the best results then switch to cpap mode & use cflex or epr (Respironics, Resmed) to ease the breathing out pressure.
A straight Bilevel (not a timed one) is in my opinion, just a cpap with a terrific EPR capability. The downside of some models is their lack of good data reporting, but again that is changing.
DSM
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): CPAP, auto, APAP
I understand an APAP can be used as a CPAP too, but I'm leary now that I've learned an APAP can't do what I thought it could do. If I'm going to use it as CPAP, why spend the money for an APAP? This has been a big eye-opener for me. I have seen a lot of posts about how the range set on an APAP is important and it's my understanding I'd learn what to set it to by looking at the software data, but if I do decide to spring for an APAP and set the low end to my current pressure and the top end 3 or 4 more than that, but it can't change pressure rapidly enough to preempt apneas, what good is it?
<<
Hi,
I think this is a misinterpretation of the discussions thus far.
AUTOs *do* pre-empt apneas. All we have been discussing in detail is how an auto might handle 'sudden' apneas (the hypothetical case mentioned) & thus far the information provided here can be taken to show that depending on exactly the circumstances, the Auto may be close enough in required pressure to make a difference or it may be succesful in preventing the next one.
The bottom line in deciding if an AUTO is good for you is how well they work for others and I think there is enough feedback here to show a lot of happy users.
One great incentive to buy an AUTO was that they provided vastly superior data to what most cpap machines did. That is changing slowly but still applies today.
>>
But I do like the idea of using an APAP in lieu of a sleep study as Ric suggested. That makes good sense. Now I have to reconsider again. This isn't an easy one to decide.
<<
Yes, this is the value proposition that AUTOs bring to the table. They can function as both AUTO and CPAP - because of this they can be used to reasses ones 90% pressure requirement whenever the user wants & if running in pure AUTO mode is not achieving the best results then switch to cpap mode & use cflex or epr (Respironics, Resmed) to ease the breathing out pressure.
A straight Bilevel (not a timed one) is in my opinion, just a cpap with a terrific EPR capability. The downside of some models is their lack of good data reporting, but again that is changing.
DSM
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): CPAP, auto, APAP
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
-
Guest
dsm wrote:AUTOs *do* pre-empt apneas. All we have been discussing in detail is how an auto might handle 'sudden' apneas (the hypothetical case mentioned) & thus far the information provided here can be taken to show that depending on exactly the circumstances, the Auto may be close enough in required pressure to make a difference or it may be succesful in preventing the next one.
This is very confusing. DSM says APAPs *do* preempt apneas. Bill says the Respironics APAP *can't* change pressure rapidly enough to preempt apneas and the data is unequivocal. Which is it? Can they or can't they?NightHawkeye wrote:I've already reached my conclusion regarding APAP's, and my conclusion is that the Respironics APAP algorithm cannot change pressure rapidly enough to pre-empt apneas. The data is unequivocal.
Bill, this is a question for you. DSM says you meant to say APAPs *do* preempt apneas but not sudden ones. Is he right? Even though your data unequivocally shows they can't?
It's had to know what to do. I had made up my mind to get the Respironics Auto until I found out about Bill's data. Then I changed my mind and decided not to spend the extra money on an APAP and just get a CPAP. Then I thought an APAP would be good for the sleep study aspect, but was disappointed to learn it couldn't preempt apneas. Now someone else says it can preempt apneas. I think I'll just go with the APAP and take my chances. If APAPs really can preempt apneas then that's what I wanted all along. I guess I reacted too fast in taking one person's word for it. This place is a great source of information and you all have been very helpful, but I'd feel a lot better about this decision if you actually agreed on whether or not an APAP can preempt an apnea. It's the biggest selling point of APAPs for me and probably for other people too.
I'm going to get the Respironics Auto with cflex. I'm almost afraid to check back here later to see what I'm going to read about it next.
Anonymous wrote:dsm wrote:AUTOs *do* pre-empt apneas. All we have been discussing in detail is how an auto might handle 'sudden' apneas (the hypothetical case mentioned) & thus far the information provided here can be taken to show that depending on exactly the circumstances, the Auto may be close enough in required pressure to make a difference or it may be succesful in preventing the next one.This is very confusing. DSM says APAPs *do* preempt apneas. Bill says the Respironics APAP *can't* change pressure rapidly enough to preempt apneas and the data is unequivocal. Which is it? Can they or can't they?NightHawkeye wrote:I've already reached my conclusion regarding APAP's, and my conclusion is that the Respironics APAP algorithm cannot change pressure rapidly enough to pre-empt apneas. The data is unequivocal.
Bill, this is a question for you. DSM says you meant to say APAPs *do* preempt apneas but not sudden ones. Is he right? Even though your data unequivocally shows they can't?
It's had to know what to do. I had made up my mind to get the Respironics Auto until I found out about Bill's data. Then I changed my mind and decided not to spend the extra money on an APAP and just get a CPAP. Then I thought an APAP would be good for the sleep study aspect, but was disappointed to learn it couldn't preempt apneas. Now someone else says it can preempt apneas. I think I'll just go with the APAP and take my chances. If APAPs really can preempt apneas then that's what I wanted all along. I guess I reacted too fast in taking one person's word for it. This place is a great source of information and you all have been very helpful, but I'd feel a lot better about this decision if you actually agreed on whether or not an APAP can preempt an apnea. It's the biggest selling point of APAPs for me and probably for other people too.
I'm going to get the Respironics Auto with cflex. I'm almost afraid to check back here later to see what I'm going to read about it next.
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
-
NightHawkeye

- Posts: 2431
- Joined: Thu Dec 29, 2005 11:55 am
- Location: Iowa - The Hawkeye State
First, I'll just add that I think the advice you've gotten from Ric and DSM regarding APAP's is good. And, like I said before, my recommendation would also be for an APAP because that is a more flexible machine which gives you more options. Apnea is tough business, and folks usually encounter many problems on their path to successful treatment. The more options you have, the more likely you are to be successful.Guest wrote:This is very confusing. DSM says APAPs *do* preempt apneas. Bill says the Respironics APAP *can't* change pressure rapidly enough to preempt apneas and the data is unequivocal. Which is it? Can they or can't they?
Bill, this is a question for you. DSM says you meant to say APAPs *do* preempt apneas but not sudden ones. Is he right? Even though your data unequivocally shows they can't?
Remember that my experience with APAP represents just a single data point, perhaps unique, perhaps not so unique. If one were to base their decision simply on my results then I'd also add that a regular CPAP would be a very poor machine for me. The reason is that, because of aerophagia, I can not endure the constant pressure of CPAP, whereas I obtain pretty decent sleep using an APAP despite the fact that a few extra apneas creep in that wouldn't with CPAP (but then I can't tolerate CPAP . . . )
Good choice. I hope the understanding gained from considering the machine limitations will help you fine tune your therapy.Guest wrote:It's had to know what to do. I had made up my mind to get the Respironics Auto until I found out about Bill's data. Then I changed my mind and decided not to spend the extra money on an APAP and just get a CPAP. Then I thought an APAP would be good for the sleep study aspect, but was disappointed to learn it couldn't preempt apneas. Now someone else says it can preempt apneas. I think I'll just go with the APAP and take my chances.
Isn't it fun though?Guest wrote:I'm going to get the Respironics Auto with cflex. I'm almost afraid to check back here later to see what I'm going to read about it next.
Regards,
Bill
-
NightHawkeye
- Posts: 2431
- Joined: Thu Dec 29, 2005 11:55 am
- Location: Iowa - The Hawkeye State
The points were taken from quite different contexts & then mixed.NightHawkeye wrote:Perhaps, but it's hard to dispute the obvious merits of the questions. .dsm wrote:Guest,
I think you are being quite mischevious
Regards,
Bill
The details of various types of pre-emption had been discussed in great length beforehand.
The meaning of the word 'apnea' (from flow limitation to blockage) as used by 'guest' is so broad that there is no sensible answer to that aspect of 'guests' question - I suspect 'guest' knew that
DSM
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
-
Guest
You would be wrong about that. I have no idea the difference from flow limitation to blockage.dsm wrote:The meaning of the word 'apnea' (from flow limitation to blockage) as used by 'guest' is so broad that there is no sensible answer to that aspect of 'guests' question - I suspect 'guest' knew that
DSM
Thanks Bill. Your honesty and willingness to explain is very much appreciated. I look to you for answers because of this and notice you are patient and helpful to others and also with me and my probably stupid questions. I think DSM is using the word mischievous instead of stupid, but I know what he meant. Anyway, thank you Bill for taking the time.NightHawkeye wrote:Remember that my experience with APAP represents just a single data point, perhaps unique, perhaps not so unique. If one were to base their decision simply on my results then I'd also add that a regular CPAP would be a very poor machine for me. The reason is that, because of aerophagia, I can not endure the constant pressure of CPAP, whereas I obtain pretty decent sleep using an APAP despite the fact that a few extra apneas creep in that wouldn't with CPAP (but then I can't tolerate CPAP . . . )
guest,
>>
Thanks Bill. Your honesty and willingness to explain is very much appreciated. I look to you for answers because of this and notice you are patient and helpful to others and also with me and my probably stupid questions. I think DSM is using the word mischievous instead of stupid, but I know what he meant. Anyway, thank you Bill for taking the time.
<<
Logging in to discussions anonymously is fine if one is asking general questions.
Logging in anonymously to detailed technical discussions and passing comments is high risk. It is challenging enough to do so with an id
It opens up questions about the posters motives.
Most people understand the basic principle that joining in a discussion with an identity is a politeness that avoids problems. It is a politeness that is very simple to undertake.
Cheers
DSM
>>
Thanks Bill. Your honesty and willingness to explain is very much appreciated. I look to you for answers because of this and notice you are patient and helpful to others and also with me and my probably stupid questions. I think DSM is using the word mischievous instead of stupid, but I know what he meant. Anyway, thank you Bill for taking the time.
<<
Logging in to discussions anonymously is fine if one is asking general questions.
Logging in anonymously to detailed technical discussions and passing comments is high risk. It is challenging enough to do so with an id
It opens up questions about the posters motives.
Most people understand the basic principle that joining in a discussion with an identity is a politeness that avoids problems. It is a politeness that is very simple to undertake.
Cheers
DSM
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
DSM, Bill, Ric, et al--I hope to return to this thread Tuesday. Unfortunately I'll perform two days of home-based client work this weekend, then jaunt the next state over to spend the holiday with extended family. Wanted to wish everyone a nice holiday weekend!
Guest(s), I hope you're still behaving when I get back.
Guest(s), I hope you're still behaving when I get back.
Last edited by -SWS on Fri May 26, 2006 9:37 pm, edited 1 time in total.
-
Guest
To DSM,dsm wrote: Logging in to discussions anonymously is fine if one is asking general questions.
Logging in anonymously to detailed technical discussions and passing comments is high risk. It is challenging enough to do so with an id
It opens up questions about the posters motives.
Most people understand the basic principle that joining in a discussion with an identity is a politeness that avoids problems. It is a politeness that is very simple to undertake.
Cheers
DSM
I have asked many questions here and in other subjects over the past few weeks and this is the first time anyone has ever asked about my motives or said I was being impolite. Bill has unequivocal data that the Respironics APAP cannot change rapidly enough to preempt apneas. You come along and say it can. When I asked for clarification, Ric and Bill helped to explain it. Everyone has been very friendly and kind and welcoming and helpful with everything I have asked. Especially Bill. I have felt welcome to ask questions --until now-- even in detailed technical discussions. That's how I've learned what I have so far. If you don't like answering technical questions then don't. It would be better not to hear from you at all, than to hear from you saying the person asking the question has questionable motives or is being impolite. That is not at all helpful. Fortunately Bill doesn't feel the same way you do or I wouldn't have learned half of what I have so far.
To Bill,
I wanted to try to thank you again. You've been very helpful and I appreciate that you have always been willing to answer my questions. I've learned a lot from you and will continue to ask questions as they come up. I look forward to getting the Respironics Auto with cflex and you are right because what I have learned here from you and Ric and SWS will help me fine tune my therapy. Thanks for taking the time.
It can.Anonymous wrote:I thought it could reach up and get what a regular CPAP couldn't.
Imagine you have a straight CPAP set at 10, say. Then you roll over in your sleep and manage to occlude your airway in a manner such that it will resist pressures up to and including 11, for example. How long before the CPAP machine is able to get you breathing again? Simple answer, it won't. You now have an apnea event that will cause an increase in arterial CO2 which will lead to a cortical arousal which will set in motion a physiological response that will eventuate into a postural rearrangement or stirring or exaggerated breathing response which will get you breathing again. CPAP is not involved. It is not ALLOWED to respond. How long does all this take? Mileage may vary.
Replay that, using an APAP set to a range of 10-16, say. Will the APAP detect the event. Hopefully. Will it respond? Probably. Can it "reach up" and attempt to deal with the situation. Certainly. Will it respond sooner than mother nature? That is where the debate lies. Does this contradict Bill's "unequivocal data"? No. Confusing? Yes.
The way I read the arguments, it is focused on a narrowly contrived situation, a sudden and large apnea, occlusive in nature, and centers on whether or not the machine can respond quickly enough to actually "prevent" an actual "apnea" as determined by the predetermined objective criteria for what will be recorded by the machine as an "actual" event having occurred. That there are indeed "tick marks" on our data somehow implies imperfection of a sort. Of course there are those pesky "centrals" that confuse the analysis. OK, the machine is allowed SOME tick marks.
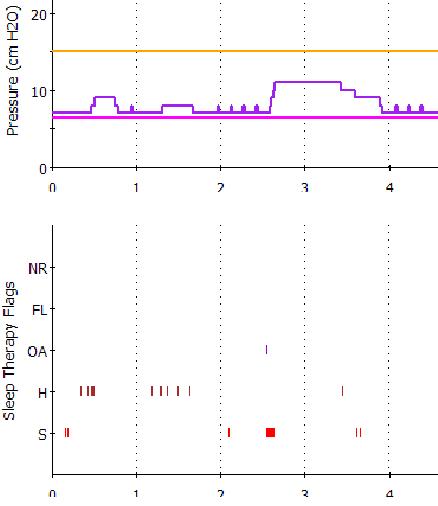
That the APAP machine responds with higher pressure, even if it's late on arrival, and that it "loiters" at a higher pressure suggests that it COULD entirely preempt SOME events, the same way a CPAP preempts apnea events (non-events?) that WOULD HAVE happened absent the air pressure. Consider the following graph, and notice an event at about 2.5 hours. this patient shows an apnea, followed by a rapid rise from 7cm to 12cm pressure, and some disgusting snore sounds early on. Note too that the pressure lingers for nearly an hour at 12cm pressure for whatever reason it's algorithm told it to. Imagine further this patient's situation on CPAP set at a constant 7cm, which just HAPPENS to correspond to this patient's sleep lab titration. Who knows how many apnea tick marks are "missing" from this data? It's hard to quantify what DIDN'T happen.
Can the APAP beat "nature" at resolving an airway occlusion, at least SOME of the time? I would argue yes. Those are impossible to measure. It would only show up as a lower AHI. That the APAP doesn't do a perfect job of what it's doing doesn't bother me. That it does an adequate job most of the time is good. Does it do a BETTER job than a CPAP? I believe it does. But that doesn't end the debate.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~
(As an aside, I have tried to imagine the "perfect" APAP device. My inclination would be to have a jury of twelve wide-awake board-certified pulmonologists monitoring every breath, each with a finger on a button to raise/lower the pressure at any given moment, with some built-in protection that it could not raise or lower more than 1cm by a simple majority vote before they were allowed another round of consensus voting. (Not even Bill Gates would spring for that, but nevermind the cost). And more than likely one would wake up to find them debating global warming or Suns vs. Mavs, etc. and neglecting your therapy. That aside, I actually think the right kind of machine might do a better job of it, when they eventually "get it right", and when these puppies become "near-sentient".)
~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Final thought, thanks to everyone, guest, bill, dsm, -SWS, myself (deep bow) and all the others who joined in making this lively and informative. I see I still have LOTS to learn. I too am 10-4, over and out (whatever THAT means) for the long weekend. Hope to be drifting lazily on an inner-tube at Lake Arrowhead thinking deep thoughts while y'allz continue to debate biophysics.
CHEERIO !
-Ric

~~~~~~~~~~~~~~~~~~~~~~~~~~~~
This holiday especially, remember the heros who gave their all to make this debate possible.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Last edited by Ric on Sat May 27, 2006 8:50 am, edited 1 time in total.
He who dies with the most masks wins.