I don't think an increase in minimum pressure is the way to go. The cpap pressure is used to help maintain or hold the airway open and thus is used for obstructive events because obstructive means the airway tissues collapse either full collapse (OA) or partial collapse (Hyponea)and thus the term obstructive. Your obstructive events (OA and Hyponeas) are already well treated.
Clear airway (centrals) are a cessation of air flow but the airway is not obstructed. There is no collapse of the airway tissues. Instead the airway is completely open but no air moves.
Hold your breath for 10 seconds. That is technically a clear airway cessation of breathing or a central.
There are a small percentage of cpap users who pressure actually will trigger more centrals. 10 to 15 % of cpap users may have this happen. It is not common but it can happen. Your "centrals" (if they are real centrals) don't appear in the first half of the night..this would be odd because if one is going to have these pressure induced centrals then logic tell us they would happen all night, not just half the night. But something to consider.
If anything...I would think about reducing the minimum.
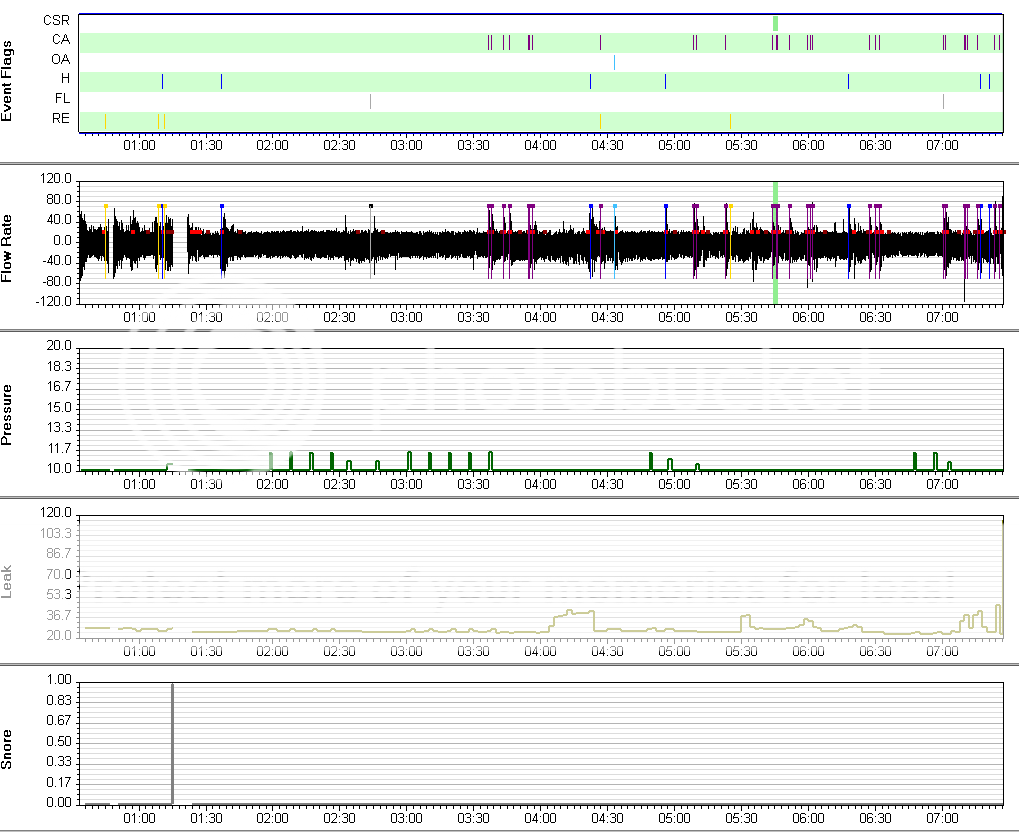
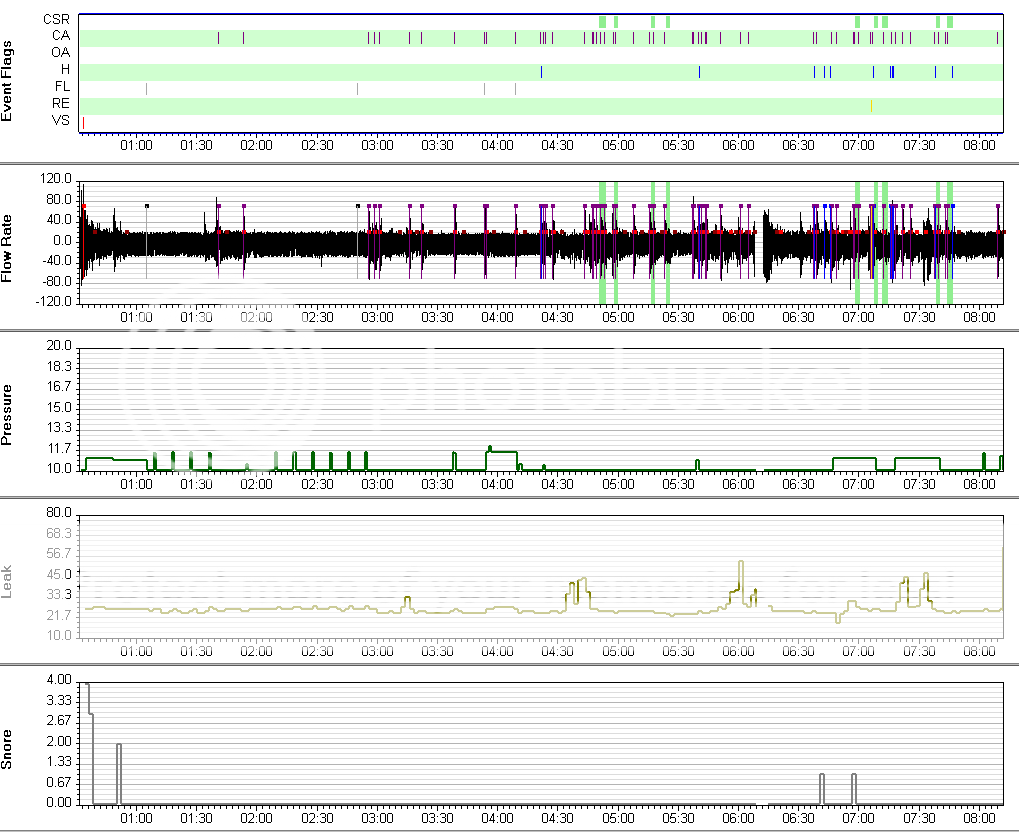
Please take the time to read this thread and click on the links to the report images. 2 pages. It will explain a bit what I am thinking.
viewtopic.php?f=1&t=68846&st=0&sk=t&sd=a I don't know that this is your situation. We don't know if you had any centrals in your sleep study.
So much we don't know and about all we do know is that those second half of the night...suck. Why? We don't know yet.
Also..just because the machine flags or scores a Clear Airway event...as Robysue has said..it doesn't mean it is/was a true central that would get us in a panic. Last night my machine flagged 18 CAs over 8 hours. A bit more than I normally see. So I went into SleepyHead and I looked at each event zoomed in to see the level of flow. Only 3 showed a flat line which meant zero flow or zero air movement. The others all had partial flow present. They didn't look like a "real" central. These machines don't have the added data available for scoring centrals. It is a one dimensional report. It gets close but the machine can't tell if you held your breath turning over in bed or even if you happened to be awake or semi awake when it is common to have sleep transition centrals.
So we can't see from your reports if these are true flat line cessation of air movement or just a reduced flow.
We will need to do more detective work.
If it were me.. I would lower the minimum to 9 and not raise the minimum at all. Your obstructives are already well treated. And the centrals (if they are true) aren't treated with increase in pressure.
I may have to RISE but I refuse to SHINE.