






Hi SU, I think Muffy probably now has all the data at hand. Its just that one epoch=30 seconds, therefore 1008 epochs x 30 seconds = 30240 seconds and with 3600 seconds/hour => 30240/3600=8.4 hours of PSG to analyse. I think that Muffy was just saying that it would take quite a while to analyse my entire sleep study epoch-by-epoch (i.e. micro analysis). Or did I miss something? Cheers,SleepingUgly wrote:BB, why don't you just mail Muffy a DVD of your sleep study? Wouldn't that be easier for both of you?Muffy wrote:One epoch down, 1007 to go. It's going to be close. Muffy
CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
-
blizzardboy

- Posts: 368
- Joined: Mon Feb 15, 2010 12:13 am
- Location: South Australia
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
Machine: Resmed VPAP Adapt SV Enhanced
Mask: Resmed Quattro/Mirage Liberty
Humidifier: Resmed H2i
Other comments: Sleepzone heated tube; CMS-50E SPO2 & CMS-60C ABPM
Mask: Resmed Quattro/Mirage Liberty
Humidifier: Resmed H2i
Other comments: Sleepzone heated tube; CMS-50E SPO2 & CMS-60C ABPM

Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
Nope, that's basically it. There is a systematic way that the data is reviewed and scored which requires setting up all the parameters, going through the study multiple times to score events (one does not generally go through epoch-by-epoch, one does all the sleep staging first, then arousals, then respiratory events, etc.). Some of these processes can be computer-scored but must be confirmed by eyeball. Then the associations are run ("this PLM has a closely-followed arousal", so it's a "PLM with arousal", etc.).blizzardboy wrote:Hi SU, I think Muffy probably now has all the data at hand. Its just that one epoch=30 seconds, therefore 1008 epochs x 30 seconds = 30240 seconds and with 3600 seconds/hour => 30240/3600=8.4 hours of PSG to analyse. I think that Muffy was just saying that it would take quite a while to analyse my entire sleep study epoch-by-epoch (i.e. micro analysis). Or did I miss something? Cheers,SleepingUgly wrote:BB, why don't you just mail Muffy a DVD of your sleep study? Wouldn't that be easier for both of you?Muffy wrote:One epoch down, 1007 to go. It's going to be close. Muffy
The program we are using is a reader-only, so it can't assist in scoring, record any scoring, perform computer scoring, do the associations or generate reports, so to actually generate a report would take about 24 hours worth of labor (like in the "good ol' days" of "paper" records)(or so I've read in the Sleep History books).
Nor does it include the sleep lab's scoring record.
Then, to top it off, after a representative epoch is found, a "snapshot" must be taken, some comments applied, and explanation of events in terms that everybody/somebody/nobody will understand must be composed.
That said, it is a great little program and does what it's designed to do.
Muffy
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
Not to mention some of the other aforementioned obstacles to overcome:
Muffy(Muffy) has the attention span of an otter on crystal meth.
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
-
blizzardboy
- Posts: 368
- Joined: Mon Feb 15, 2010 12:13 am
- Location: South Australia
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
Muffy wrote:Not to mention some of the other aforementioned obstacles to overcome:(Muffy) has the attention span of an otter on crystal meth.
Machine: Resmed VPAP Adapt SV Enhanced
Mask: Resmed Quattro/Mirage Liberty
Humidifier: Resmed H2i
Other comments: Sleepzone heated tube; CMS-50E SPO2 & CMS-60C ABPM
Mask: Resmed Quattro/Mirage Liberty
Humidifier: Resmed H2i
Other comments: Sleepzone heated tube; CMS-50E SPO2 & CMS-60C ABPM
-
SleepingUgly

- Posts: 4690
- Joined: Sat Nov 28, 2009 9:32 pm
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
BB, could you ask Mother whether, at her lab, she uses the Chicago Criteria, the AASM recommended, or the AASM alternative criteria for scoring hypopneas?
_________________
| Mask: Swift™ FX For Her Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Rescan 3.10 |
Never put your fate entirely in the hands of someone who cares less about it than you do. --Sleeping Ugly
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
I certainly hope you have reserved the name "MethOtter" for when "Muffy" approaches 1,000 posts.Muffy wrote:Not to mention some of the other aforementioned obstacles to overcome:
Muffy(Muffy) has the attention span of an otter on crystal meth.
Perhaps this guy can sculpt you a custom-made avatar . . .
https://www.youtube.com/watch?v=x75jAx1Pbys
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
+1blizzardboy wrote:I can't tell you how much I appreciate your time and effort Muffy.Muffy wrote:One epoch down, 1007 to go. It's going to be close.
It has to be one of those last two since Muffy runs an AASM accredited sleep center.SleepingUgly wrote:Muffy, when you score hypopneas, do you use the Chicago Criteria, the AASM Recommended, or the AASM Alternative criteria?
-
SleepingUgly
- Posts: 4690
- Joined: Sat Nov 28, 2009 9:32 pm
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
I don't think scoring things according to the AASM guidelines is criteria for accreditation.-SWS wrote:It has to be one of those last two since Muffy runs an AASM accredited sleep center.SleepingUgly wrote:Muffy, when you score hypopneas, do you use the Chicago Criteria, the AASM Recommended, or the AASM Alternative criteria?
_________________
| Mask: Swift™ FX For Her Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Rescan 3.10 |
Never put your fate entirely in the hands of someone who cares less about it than you do. --Sleeping Ugly
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
See Section F-2 on PDF page 23 of 31 here, SU:SleepingUgly wrote:I don't think scoring things according to the AASM guidelines is criteria for accreditation.-SWS wrote:It has to be one of those last two since Muffy runs an AASM accredited sleep center.SleepingUgly wrote:Muffy, when you score hypopneas, do you use the Chicago Criteria, the AASM Recommended, or the AASM Alternative criteria?
http://www.aasmnet.org/Resources/PDF/De ... ndards.pdf
It seems "AASM recommended" scoring is required for accreditation as an "AASM sleep center". I didn't know that until just having looked it up via Mr. Google... So if Muffy is behaving according to AASM sleep center requirements, then I think she uses the "AASM recommended" hypopnea scoring standards.
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
Well, interesting that you guys should be talking about rules, cause that's going to play a key role in the next area of analysis.
That area at about 0330 deserves a special look, because that's where they scored a bunch of obstructive apneas:
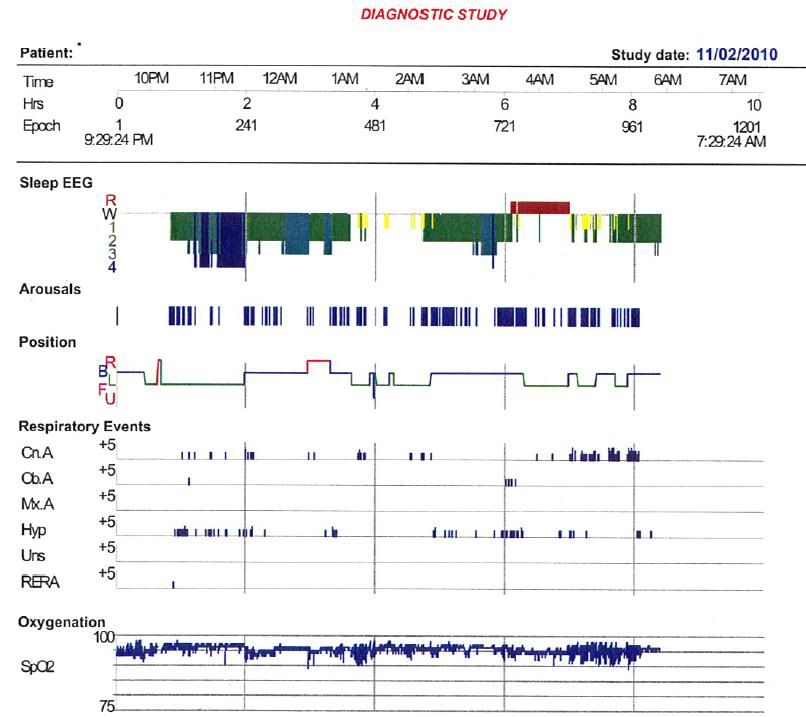
Now, with a bunch of obstructive apneas, a diagnosis of "Obstructive Sleep Apnea" becomes a heckuva lot more plausible (for obvious reasons).
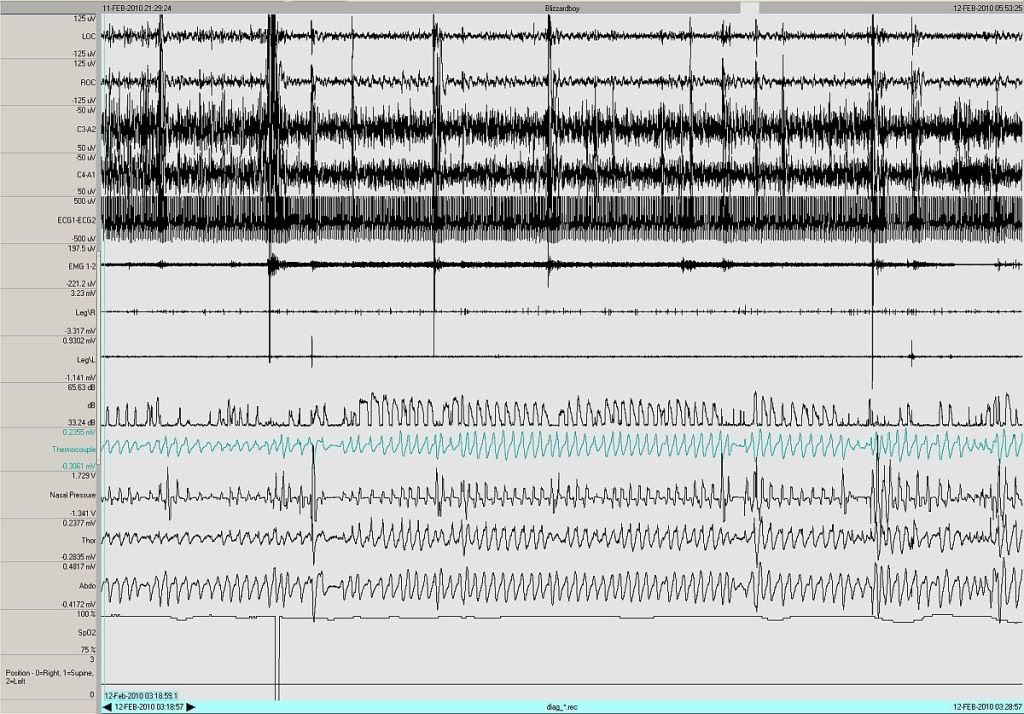
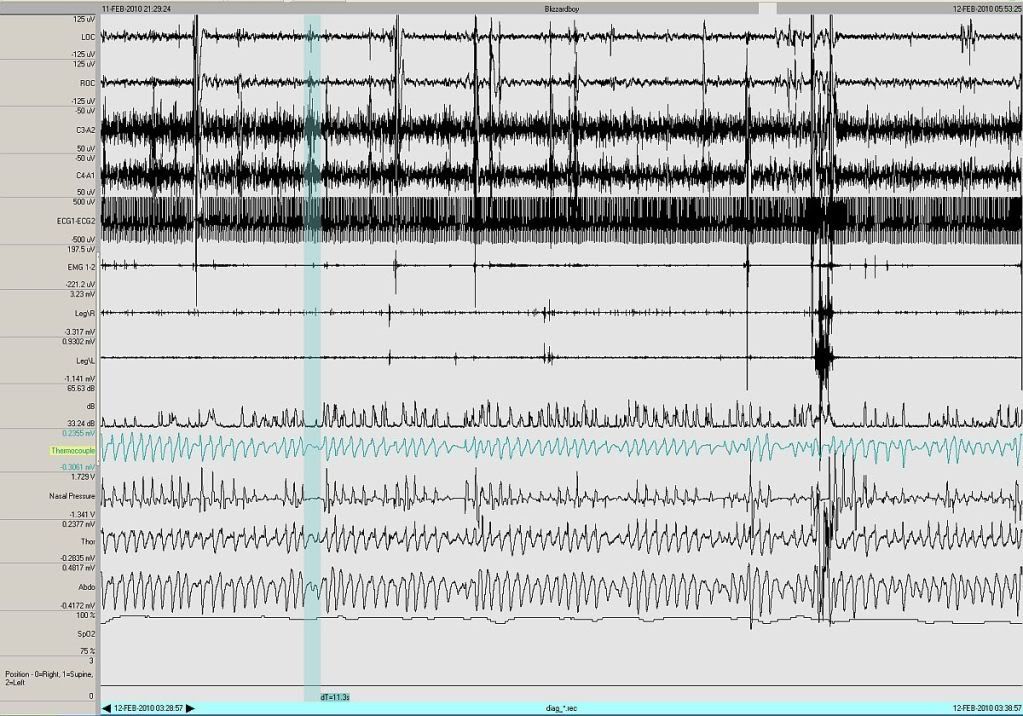
However, we have the raw data to see exactly what was happening in that area. Here's a total of 10 minutes during that stretch, which I believes covers the entire "obstructive" area:
I think it's academic.
What would you use here?
Muffy
That area at about 0330 deserves a special look, because that's where they scored a bunch of obstructive apneas:
Now, with a bunch of obstructive apneas, a diagnosis of "Obstructive Sleep Apnea" becomes a heckuva lot more plausible (for obvious reasons).
However, we have the raw data to see exactly what was happening in that area. Here's a total of 10 minutes during that stretch, which I believes covers the entire "obstructive" area:
SleepingUgly wrote:Muffy, when you score hypopneas, do you use the Chicago Criteria, the AASM Recommended, or the AASM Alternative criteria?
I think it's academic.
What would you use here?
Muffy
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
"The AASM recently published the Manual for the Scoring of Sleep and Associated Events. In this manual there is a “recommended” and an “alternative” hypopnea definition; and either can be used at the discretion of the clinician or investigator."--http://www.ncbi.nlm.nih.gov/pmc/article ... .2.150.pdf
"Each AHI reported should be based on consistent application of either rule 4a or 4b. Scoring using 4a and 4b cannot be combined to compute a single AHI. Laboratories that choose to use both rules must report AHI for each rule separately."--http://www.aasmnet.org/SMFAQs.aspx
"The AASM Manual for the Scoring of Sleep and Related Events is not a guideline or practice parameter, and uses slightly different terminology. The key on page 15 indicates that "recommended," "alternative," and "optional" rules are all methods acceptable by AASM for scoring. An accredited center must follow all of the rules, but based on the discretion of the clinician or investigator a specific center may use "alternative" or "optional" rules in the place of the "recommended" rule. The use of "alternative" or "optional" rules would not create any risk to accreditation."--http://www.aasmnet.org/Resources/PDF/FA ... Manual.pdf

Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
JNKjnk wrote:"The AASM recently published the Manual for the Scoring of Sleep and Associated Events. In this manual there is a “recommended” and an “alternative” hypopnea definition; and either can be used at the discretion of the clinician or investigator."--http://www.ncbi.nlm.nih.gov/pmc/article ... .2.150.pdf"Each AHI reported should be based on consistent application of either rule 4a or 4b. Scoring using 4a and 4b cannot be combined to compute a single AHI. Laboratories that choose to use both rules must report AHI for each rule separately."--http://www.aasmnet.org/SMFAQs.aspx"The AASM Manual for the Scoring of Sleep and Related Events is not a guideline or practice parameter, and uses slightly different terminology. The key on page 15 indicates that "recommended," "alternative," and "optional" rules are all methods acceptable by AASM for scoring. An accredited center must follow all of the rules, but based on the discretion of the clinician or investigator a specific center may use "alternative" or "optional" rules in the place of the "recommended" rule. The use of "alternative" or "optional" rules would not create any risk to accreditation."--http://www.aasmnet.org/Resources/PDF/FA ... Manual.pdf
That last link is very informative and solves a few issues I had in regard to certain types of events as it lays out the AASM approach to scoring which is acceptable to me. This doc could have save a lot of pain back a few months in some other threads
Thanks for the link.
DSM
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
Glad someone found it helpful.dsm wrote: . . . Thanks for the link.
DSM
I can't claim to understand much of that stuff. All I get from it is: "When you test, try to figure out if the patient has a problem. If you're pretty sure the patient does, then use whatever scoring criteria will get insurance to pay for treatment."
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
Chancellor JNK, you're a champ... Thanks for finding that. SU, good point. I think you were getting at what Jeff managed to find in print.
So how common is blizzardboy's PSG presentation, Muffy? There's a lot going on---plenty related to arousals.
Muffy wrote:Well, interesting that you guys should be talking about rules, cause that's going to play a key role in the next area of analysis.
That area at about 0330 deserves a special look, because that's where they scored a bunch of obstructive apneas:
Now, with a bunch of obstructive apneas, a diagnosis of "Obstructive Sleep Apnea" becomes a heckuva lot more plausible (for obvious reasons).
However, we have the raw data to see exactly what was happening in that area. Here's a total of 10 minutes during that stretch, which I believes covers the entire "obstructive" area:
SleepingUgly wrote:Muffy, when you score hypopneas, do you use the Chicago Criteria, the AASM Recommended, or the AASM Alternative criteria?
I think it's academic.
What would you use here?
Muffy
Meaning a challenge by any set of scoring standards...? Or meaning the same underlying SDB event/condition is manifest regardless of what you decide to call it?Muffy wrote:I think it's academic.
So how common is blizzardboy's PSG presentation, Muffy? There's a lot going on---plenty related to arousals.
Last edited by -SWS on Wed May 26, 2010 8:24 pm, edited 1 time in total.
Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
According to this chart, it's all a matter of simple yes-or-no questions (or in one apparent typo, no-or-no questions) once you do CPAP and a follow-up Epworth.
I had no idea it was all supposed to be this simple!:
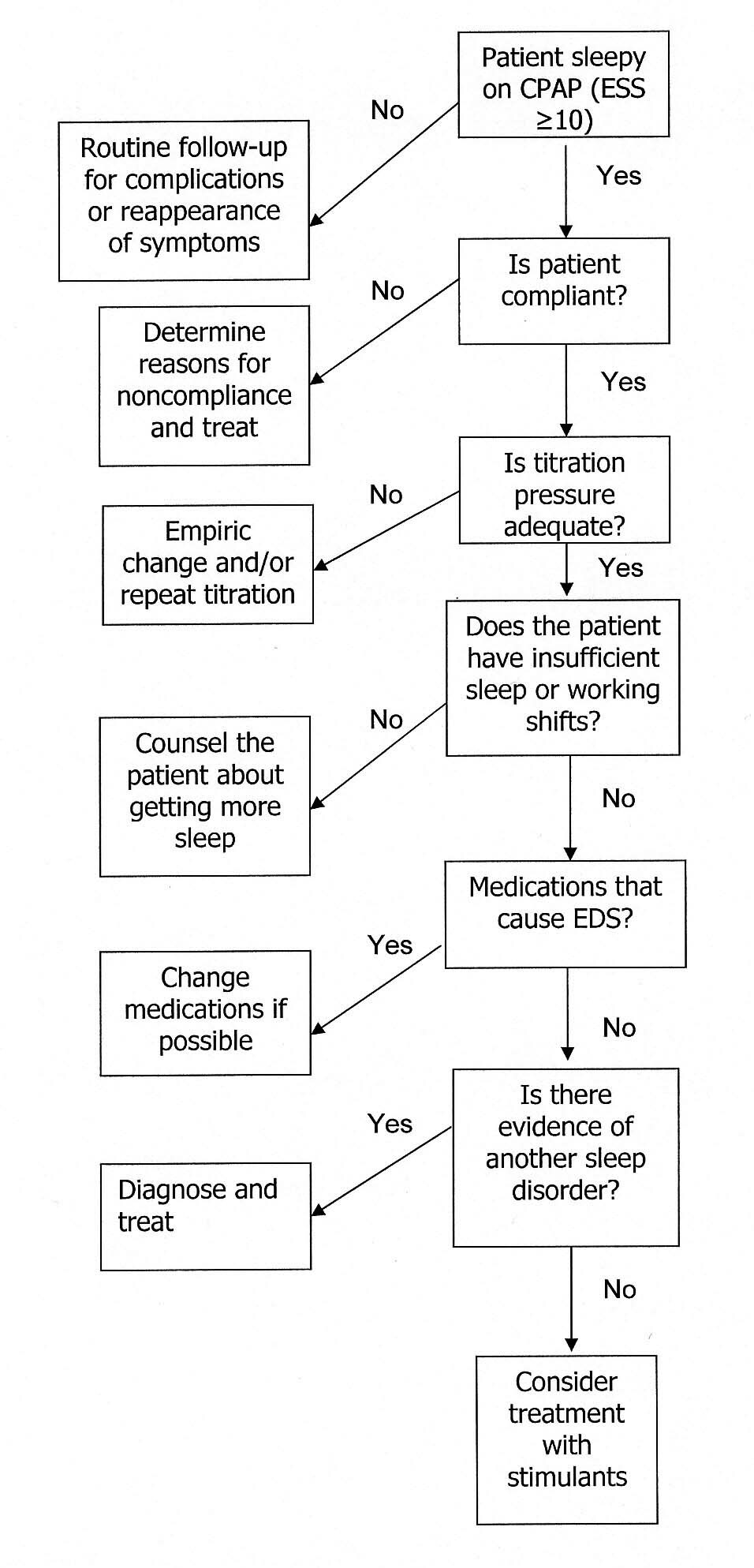
I had no idea it was all supposed to be this simple!: