






Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
-
SaltLakeJan
- Posts: 776
- Joined: Sat Jan 17, 2009 8:49 pm
- Location: Salt Lake City, Utah
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Additional Comments: Began CPAP 1-16-2009, Pressure=10 cm, Mask, CMS 50Plus Oximeter |
-
SaltLakeJan
- Posts: 776
- Joined: Sat Jan 17, 2009 8:49 pm
- Location: Salt Lake City, Utah
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Additional Comments: Began CPAP 1-16-2009, Pressure=10 cm, Mask, CMS 50Plus Oximeter |
-
SaltLakeJan
- Posts: 776
- Joined: Sat Jan 17, 2009 8:49 pm
- Location: Salt Lake City, Utah
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Additional Comments: Began CPAP 1-16-2009, Pressure=10 cm, Mask, CMS 50Plus Oximeter |
-
SaltLakeJan
- Posts: 776
- Joined: Sat Jan 17, 2009 8:49 pm
- Location: Salt Lake City, Utah
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Additional Comments: Began CPAP 1-16-2009, Pressure=10 cm, Mask, CMS 50Plus Oximeter |
-
robertmarilyn

- Posts: 523
- Joined: Sat Mar 14, 2009 7:38 pm
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
You trying to teach Muffy a lesson for his/her rant about graphs?
Last edited by robertmarilyn on Mon May 11, 2009 5:26 pm, edited 1 time in total.
-
SaltLakeJan
- Posts: 776
- Joined: Sat Jan 17, 2009 8:49 pm
- Location: Salt Lake City, Utah
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Additional Comments: Began CPAP 1-16-2009, Pressure=10 cm, Mask, CMS 50Plus Oximeter |
-
SaltLakeJan
- Posts: 776
- Joined: Sat Jan 17, 2009 8:49 pm
- Location: Salt Lake City, Utah
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
MUFFY, I'VE PUT THIS #@*! THING IN 3 TIMES, EACH TIME I GET HALF A SHEET, BUT WHEN I HIT "EXPAND VIEW"
IT EXPANDS TO FULL SIZE. Sssssssssory it is such a mess. jan
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Additional Comments: Began CPAP 1-16-2009, Pressure=10 cm, Mask, CMS 50Plus Oximeter |
-
SaltLakeJan
- Posts: 776
- Joined: Sat Jan 17, 2009 8:49 pm
- Location: Salt Lake City, Utah
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?

_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Additional Comments: Began CPAP 1-16-2009, Pressure=10 cm, Mask, CMS 50Plus Oximeter |
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
robertmarilyn wrote:You trying to teach Muffy a lesson for his/her rant about graphs?
Muffy will never want for graphs again...
-
SaltLakeJan
- Posts: 776
- Joined: Sat Jan 17, 2009 8:49 pm
- Location: Salt Lake City, Utah
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
Muffy, Sag & SWS,
Muffy you wanted graphs, I intended to get every graph posted. But, I have never read anything as funny as Muffy's post, and laughed so hard DH thought I was choking, I pointed to the screen and he is still ROTFL , so am I. Jan
EDWARD YOU IDIOT!! I SENT YOU OUT FOR GRAPHS AND YOU COME BACK WITH NUMBERS?!! I DON'T WANT NUMBERS!! IF I WANTED NUMBERS, I WOULD HAVE SAID, "EDWARD, GET ME NUMBERS!!" DID I SAY, "EDWARD, GET ME NUMBERS!!"? NO!? THEN WHY ARE YOU GIVING ME !*#%ING NUMBERS? IF I WANTED !*#%ING NUMBERS THEN I WOULD HAVE SAID "EDWARD, GET ME SOME !*#%ING NUMBERS!" BUT I DIDN'T, DID I? SO STOP WITH THE !*#%ING NUMBERS AND GET ME THE !*#%ING GRAPHS!!
BTW Jan, did you have a pleasant Mother's Day? I sure did, it was a beautiful day here, spent a lot of time outside, planted a few flowers, did a little light pruning and ripped out two tree stumps. Well, that was really all the same project. I planted the flowers in the early morning, but wouldn't you know it, by 10 AM they were covered by the shade from two big cedar trees! OK, no problem, a little pruning, and there! My new little children were back in the warm sunshine!!
Then about 2 PM, I went back out, and my poor children were again cloaked in darkness! Fine I said, and proceeded to take off a couple of branches. Great. See? Muffy can deal with adversity! No problem! Things are much better with the new medication!
But then at 5 o'clock THOSE !*#%ING TREES WERE KILLING MY PLANTS AGAIN! "OH YEAH?" I SAID AND WITH THAT I GRABBED THE OL' HUSQVARNA CHAIN SAW AND SAID "JUST WHAT THE !*#% IS YOUR PROBLEM THAT YOU CAN'T PUT A 'U' AFTER THE 'Q'" SO INSTEAD I SMASHED THE CHAINSAW TO BITS WITH A SLEDGEHAMMER AND RAMMED THE SILVERADO AT ABOUT 50 MILES AN HOUR INTO THOSE !*#%ING TREES 42 TIMES UNTIL THEY UNROOTED...
...and now my little babies are back in the sunlight again!
So what did you do?
Muffy[/quote]
Muffy, I did sent a bunch. Some are kinda screwed-up. Jan
Muffy you wanted graphs, I intended to get every graph posted. But, I have never read anything as funny as Muffy's post, and laughed so hard DH thought I was choking, I pointed to the screen and he is still ROTFL , so am I. Jan
EDWARD YOU IDIOT!! I SENT YOU OUT FOR GRAPHS AND YOU COME BACK WITH NUMBERS?!! I DON'T WANT NUMBERS!! IF I WANTED NUMBERS, I WOULD HAVE SAID, "EDWARD, GET ME NUMBERS!!" DID I SAY, "EDWARD, GET ME NUMBERS!!"? NO!? THEN WHY ARE YOU GIVING ME !*#%ING NUMBERS? IF I WANTED !*#%ING NUMBERS THEN I WOULD HAVE SAID "EDWARD, GET ME SOME !*#%ING NUMBERS!" BUT I DIDN'T, DID I? SO STOP WITH THE !*#%ING NUMBERS AND GET ME THE !*#%ING GRAPHS!!
BTW Jan, did you have a pleasant Mother's Day? I sure did, it was a beautiful day here, spent a lot of time outside, planted a few flowers, did a little light pruning and ripped out two tree stumps. Well, that was really all the same project. I planted the flowers in the early morning, but wouldn't you know it, by 10 AM they were covered by the shade from two big cedar trees! OK, no problem, a little pruning, and there! My new little children were back in the warm sunshine!!
Then about 2 PM, I went back out, and my poor children were again cloaked in darkness! Fine I said, and proceeded to take off a couple of branches. Great. See? Muffy can deal with adversity! No problem! Things are much better with the new medication!
But then at 5 o'clock THOSE !*#%ING TREES WERE KILLING MY PLANTS AGAIN! "OH YEAH?" I SAID AND WITH THAT I GRABBED THE OL' HUSQVARNA CHAIN SAW AND SAID "JUST WHAT THE !*#% IS YOUR PROBLEM THAT YOU CAN'T PUT A 'U' AFTER THE 'Q'" SO INSTEAD I SMASHED THE CHAINSAW TO BITS WITH A SLEDGEHAMMER AND RAMMED THE SILVERADO AT ABOUT 50 MILES AN HOUR INTO THOSE !*#%ING TREES 42 TIMES UNTIL THEY UNROOTED...
...and now my little babies are back in the sunlight again!
So what did you do?
Muffy[/quote]
Muffy, I did sent a bunch. Some are kinda screwed-up. Jan
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Additional Comments: Began CPAP 1-16-2009, Pressure=10 cm, Mask, CMS 50Plus Oximeter |

The Saga of SLJ: 40 Years In The Desert
Prologue
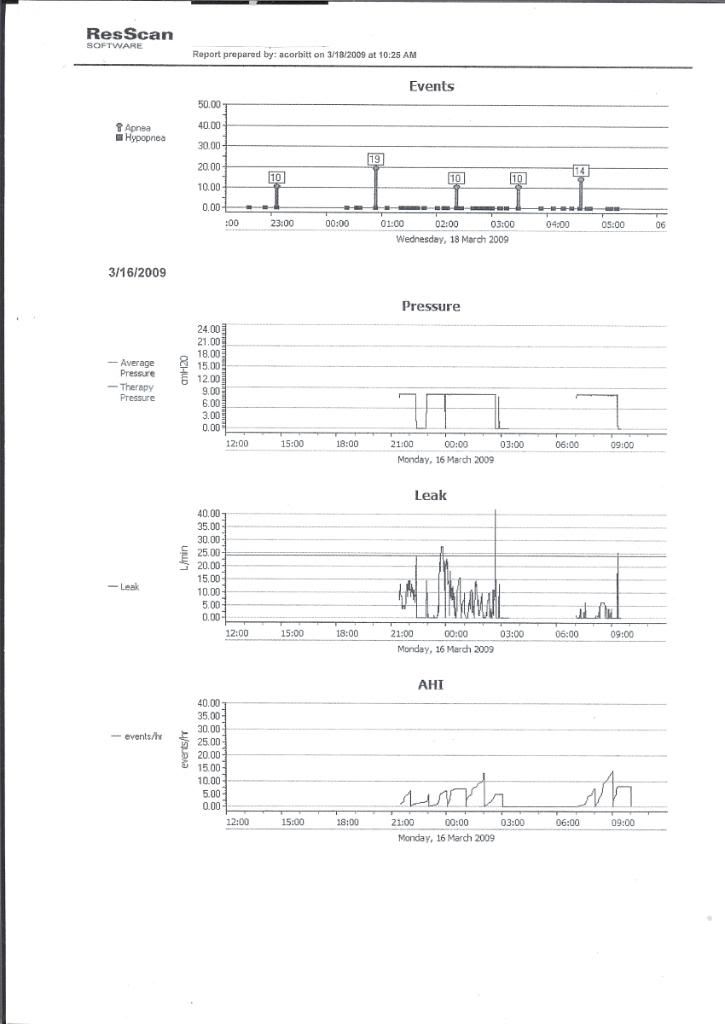
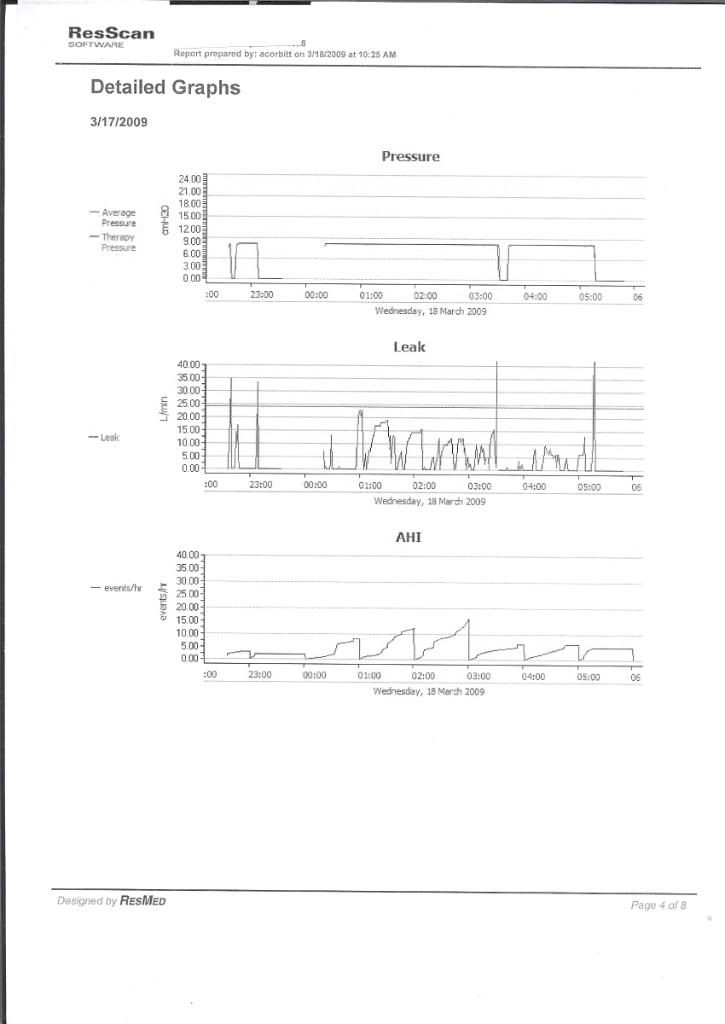
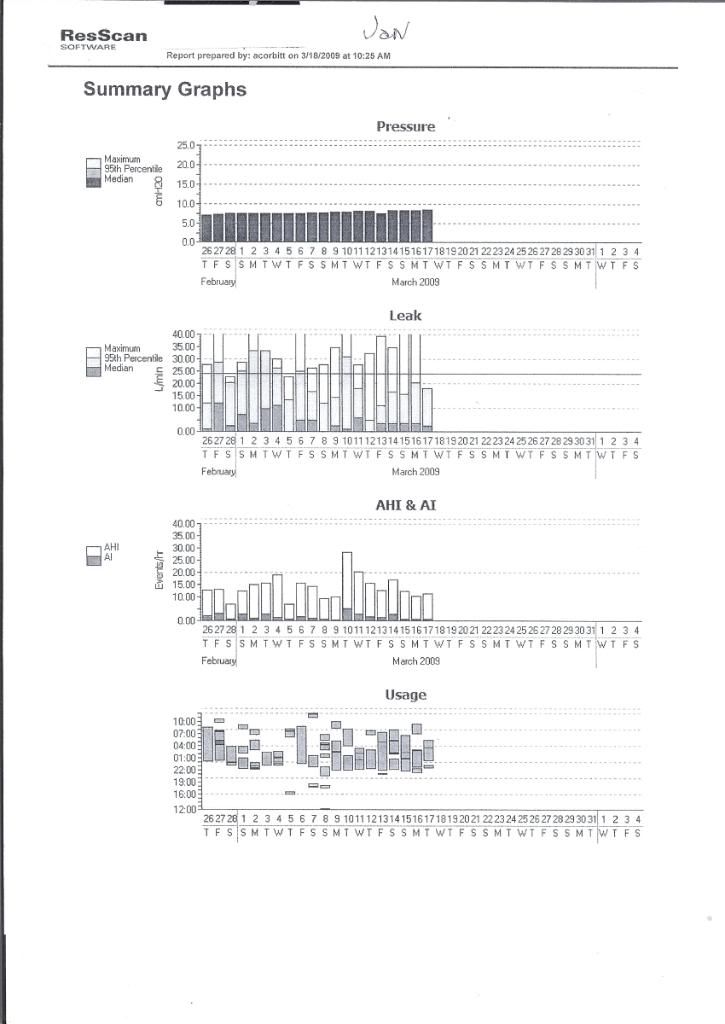
However, in response to that point, each of these graphs is a summary or 900 pages of data, so even they may not give the true picture, and in some areas, I don't believe they do.
In regards to whether or not Muffy is a well-qualified clinician, we should let her comments stand on their own merit, for as this former poster noted:
Chapter One
I think one needs to begin by examining the data presented with a critical eye as to it's basic validity and to ascertain the effect of confounding factors, assessing each study individually, determining:
Are raw data signals (such as oximetry and heart rate) accurate, or contaminated by artifact or improper acquisition settings?
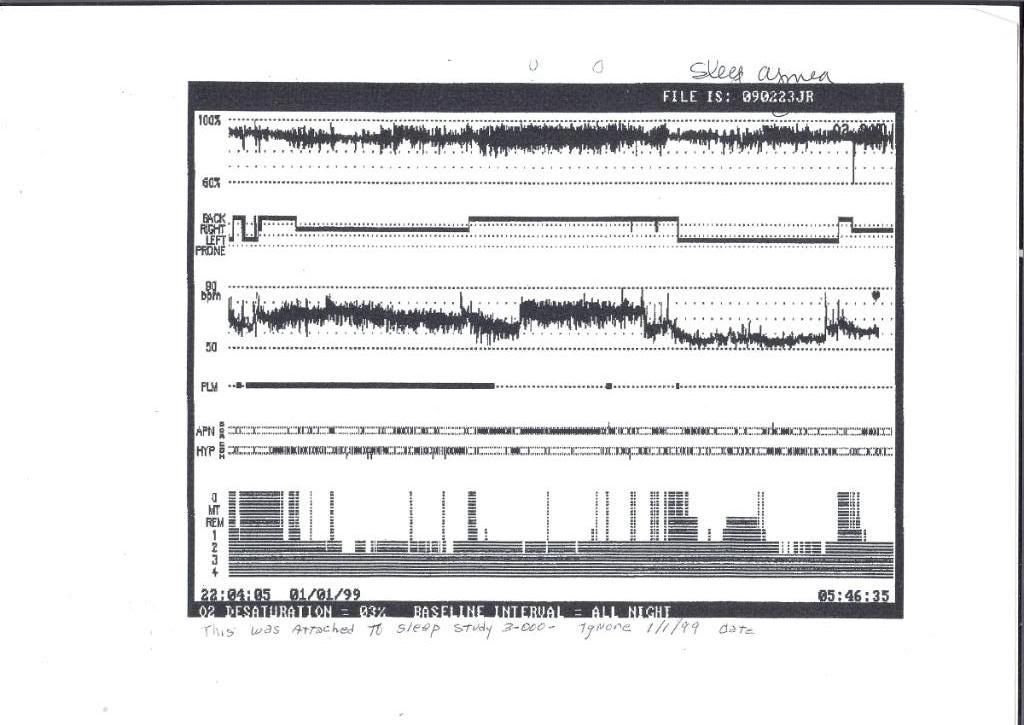
For example, that first study (the report from a "dot-matrix printer")(OK, maybe "cheap" does not necessarily mean "inaccurate") demonstrates severe heart rate variation (HRV) with the supposed respiratory events, yet this is not duplicated in the 4/25/2000 study. The well-defined and abrupt increase in baseline HR in the middle of the night is, at the least, curious. Since the oximetry signal probably also produced the heart rate signal, is 3/2000 heavily contaminated with artifact? This data on ambient pressure is a key component to understanding the underlying processes.
Are those events requiring interpretation properly scored?
Including sleep staging, arousals, PLMs (were they really PLMs?) and respiratory events. Did the first study, in fact, have a "central flavor"? Did sleep fragmentation and arousals generate events (but certainly breathing instability) rather than the other way around? I think that raw data would need to be put under the microscope, but given the passage of time, surgery and an entirely new medication cocktail, that would be academic. New ambient data is crucial to understanding here, so let me be clear-- 12/18/2008 was completely without CPAP?
If there was no application of CPAP, then how was a pressure of 10 cmH20 determined?
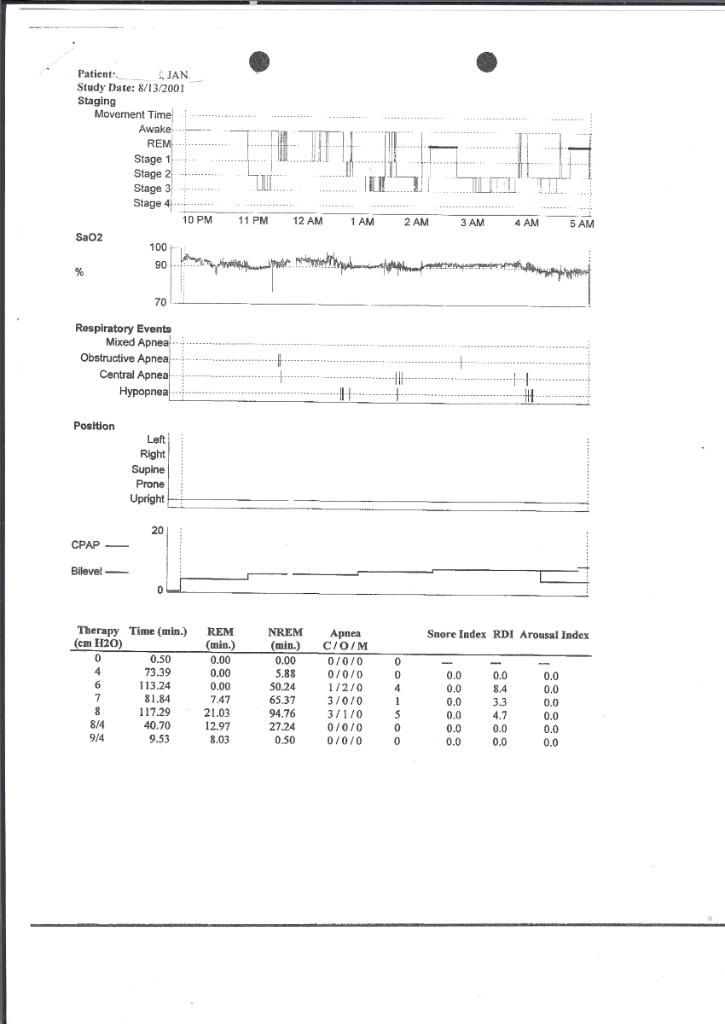
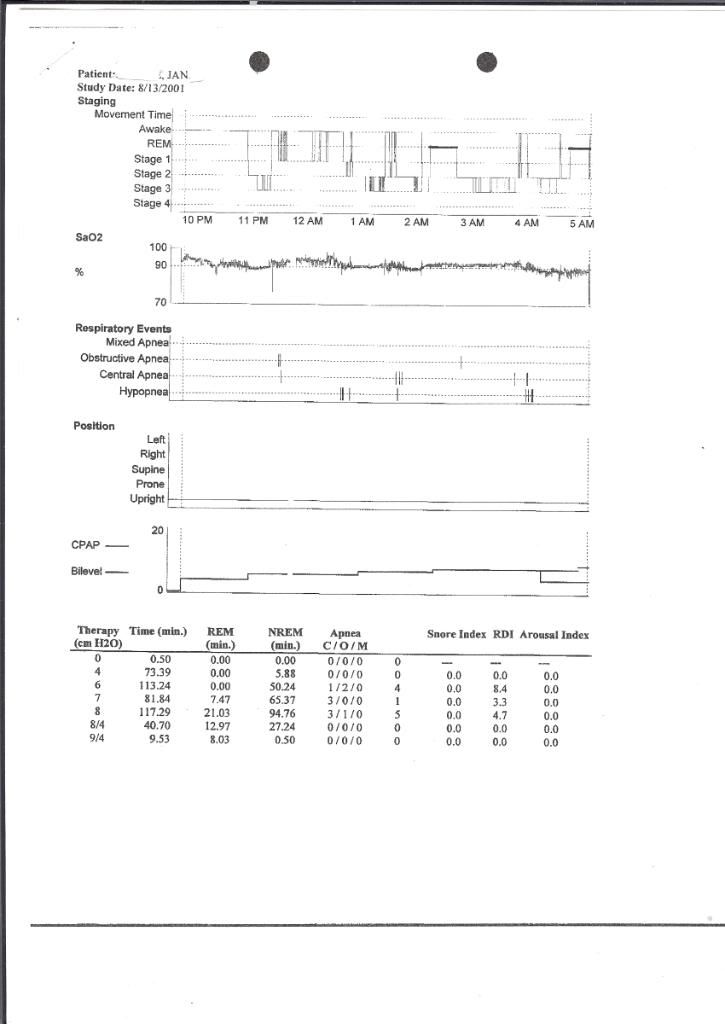
The 8/2001 Titration has some good results. Although there is considerable wake, there is good control of respiratory events at almost all pressures. The BiPAP trial looks very nice. However, the oxygen baseline is a little low, hovering near 90% should be avoided, and supplemental oxygen should be considered to get it to >~93%. Reimbursement is strict, but that tail end of the study looks like it may make you qualify. REM is significantly delayed. That early morning awakening broke into the final REM period (poor form). The position sensor appears to be inaccurate.
BTW, the whole PLM thing needs careful review. In 3/2000, the clonazapam you were taking should have had an ameliorating effect on the PLMs. As previously noted, PLMs cannot be associated with respiratory events, otherwise they aren't PLMs. To repeat my previous question:
The 12/2008 study purports
What is the effect of the medications on each study?
As an example, Effexor and Ritalin can have a very damaging effect on sleep architecture.
Are her histories and transcriptions of data accurate and complete?
For instance, in earlier posts, she notes being on Mirapex 300 mg. At that dosage, she'd have a campsite in front of the slots at Foxwoods-Mohegan Sun. Typos are important.
We need an accurate list of medications taken during each study, as well as eventually getting all this stuff into some semblance of organization (maybe by about Chapter 25).
Muffy
In as much as this thread is going to get a lot more confusing before if gets much clearer (if at all), it would be best to simply refer to Muffy as "Muffy", "Muffmeister", "The Muffburger", "Muffenstein" or "TPFKATPFKAS" with "her" comments.-SWS wrote:Because SAG/Muffy is such a well-qualified clinician, I like to "sit tight" and simply follow along as he offers his typically sharp clinical analysis.
See, whenever I see "robertmarilyn", it's tough to visualize what she looks like.robertmarilyn wrote:You trying to teach Muffy a lesson for his/her rant about graphs?
However, in response to that point, each of these graphs is a summary or 900 pages of data, so even they may not give the true picture, and in some areas, I don't believe they do.
In regards to whether or not Muffy is a well-qualified clinician, we should let her comments stand on their own merit, for as this former poster noted:
Since we now have some data to view, it might be a good idea to present these links and thoughts:StillAnotherGuest wrote:"IMHO", its not the letters anyway. Letters are not required to say something intelligent nor a guarantee that what will be said won't be stupid.
to see if they are pertinent.-SWS wrote:In light of the observations above, and the CFS diagnosis that Jan received, I have some interesting supporting links and pathophysiologic conjecture about hyperactive cognition-based arousals possibly having some degree of interrelatedness in neurology between overlapping CFS pathology and that of CompSAS/CSDB. Also a comment about a possible neurological stimulus/response mechanism that just may exist as an interrelated cohort for this particular hypothetical patient phenotype in neurology.
Chapter One
I think one needs to begin by examining the data presented with a critical eye as to it's basic validity and to ascertain the effect of confounding factors, assessing each study individually, determining:
Are raw data signals (such as oximetry and heart rate) accurate, or contaminated by artifact or improper acquisition settings?
For example, that first study (the report from a "dot-matrix printer")(OK, maybe "cheap" does not necessarily mean "inaccurate") demonstrates severe heart rate variation (HRV) with the supposed respiratory events, yet this is not duplicated in the 4/25/2000 study. The well-defined and abrupt increase in baseline HR in the middle of the night is, at the least, curious. Since the oximetry signal probably also produced the heart rate signal, is 3/2000 heavily contaminated with artifact? This data on ambient pressure is a key component to understanding the underlying processes.
Are those events requiring interpretation properly scored?
Including sleep staging, arousals, PLMs (were they really PLMs?) and respiratory events. Did the first study, in fact, have a "central flavor"? Did sleep fragmentation and arousals generate events (but certainly breathing instability) rather than the other way around? I think that raw data would need to be put under the microscope, but given the passage of time, surgery and an entirely new medication cocktail, that would be academic. New ambient data is crucial to understanding here, so let me be clear-- 12/18/2008 was completely without CPAP?
The Oxygen Saturation axis there is screwy (the 70% to 100% lines, are they 5% or 10% thresholds, I think they're 10s, back to that later). There seems to be a heavy supine dependency.12.08.2008 Report wrote:Pt was not split due to the amount of (night technician perceived) events seen throughout the night.
If there was no application of CPAP, then how was a pressure of 10 cmH20 determined?
The 8/2001 Titration has some good results. Although there is considerable wake, there is good control of respiratory events at almost all pressures. The BiPAP trial looks very nice. However, the oxygen baseline is a little low, hovering near 90% should be avoided, and supplemental oxygen should be considered to get it to >~93%. Reimbursement is strict, but that tail end of the study looks like it may make you qualify. REM is significantly delayed. That early morning awakening broke into the final REM period (poor form). The position sensor appears to be inaccurate.
BTW, the whole PLM thing needs careful review. In 3/2000, the clonazapam you were taking should have had an ameliorating effect on the PLMs. As previously noted, PLMs cannot be associated with respiratory events, otherwise they aren't PLMs. To repeat my previous question:
Starting out with 3.0 mg of Mirapex is pretty aggressive.Muffy wrote:but theSaltLakeJan wrote:My sleep tests were in May 2000,I have a list of the prescriptions I took for FMS/CF 3-2000 to 9-2000
Clonazapam 0.5 mg For Insomnia
Neurontin 300 mg Ambien 5 mg
Prilosec 20 mg Trazadone 100 mg
Effexor 75 mg
And based on that you went on 3.0 mg of Mirapex? What was the rationale for starting Mirapex and when did you start it?NPSG 3/3/00 wrote: LEG MOVEMENTS: Patient was noted to have 62 leg movements per hr of sleep. Most were associated with respiratory arousals.
The 12/2008 study purports
and then includes an epoch of SWS with alpha intrusion.12.8.2008 wrote:Technologist Comments: Pt a baseline study, no alpha intrusion
What is the effect of the medications on each study?
As an example, Effexor and Ritalin can have a very damaging effect on sleep architecture.
Are her histories and transcriptions of data accurate and complete?
For instance, in earlier posts, she notes being on Mirapex 300 mg. At that dosage, she'd have a campsite in front of the slots at Foxwoods-Mohegan Sun. Typos are important.
We need an accurate list of medications taken during each study, as well as eventually getting all this stuff into some semblance of organization (maybe by about Chapter 25).
Muffy
Last edited by Muffy on Tue May 12, 2009 7:01 am, edited 1 time in total.
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Re: The Saga of SLJ: 40 Years In The Desert
That's Muffin' to write home about (The Person Formerly Known As The Person Formerly Known As SAG)!Muffy wrote:Prologue
In as much as this thread is going to get a lot more confusing before if gets much clearer (if at all), it would be best to simply refer to Muffy as "Muffy", "Muffmeister", "The Muffburger", "Muffenstein" or "TPFKATPFKAS" with "her" comments.-SWS wrote:Because SAG/Muffy is such a well-qualified clinician, I like to "sit tight" and simply follow along as he offers his typically sharp clinical analysis.
I'm thinking that while some charts will clearly be inconclusive, there will be salient clues to pick out and explore. Two patterned traits that I just so happen to tentatively have my eye peeled for are: 1) temporal characteristics of atypical cognitive and CNS variability (that can longitudinally manifest as atypical CNS variability), and 2) a possibly heightened cognitive arousability trait, that can be impacted by a variety of environmental, physiological, and psychological stimuli.Muffy wrote:However, in response to that point, each of these graphs is a summary or 900 pages of data, so even they may not give the true picture, and in some areas, I don't believe they do.robertmarilyn wrote:You trying to teach Muffy a lesson for his/her rant about graphs?
An unusually heightened arousability trait of cognition is thought to be more common in the HSP, ADHD, intellectually gifted, and perhaps the CFS populations (I'll expand that statement with more links later). Anyway, I have a working theory that some people presenting heightened-arousibility traits in cognition will often present: 1) more extreme CNS variability than most people, 2) more wake-to-stage-one sleep transition problems than most people (including insomnia), and 3) perhaps even a greater tendency toward CompSAS/CSDB maladaptation when presented with CPAP stimuli intended to resolve concomitant sleep apnea.
One Very Interesting Chronic Fatigue Syndrome Theory
Re: The Saga of SLJ: 40 Years In The Desert
I think we're going to need the heart rate graphs (not the text) from the two most recent studies (2001 and 2008) in order to consider that approach and try to glean out HRV data, demonstrate that SLJ indeed has CFS or FBM, and somehow account for medication effect.-SWS wrote:Anyway, I have a working theory that some people presenting heightened-arousibility traits in cognition will often present: 1) more extreme CNS variability than most people, 2) more wake-to-stage-one sleep transition problems than most people (including insomnia), and 3) perhaps even a greater tendency toward CompSAS/CSDB maladaptation when presented with CPAP stimuli intended to resolve concomitant sleep apnea.
One Very Interesting Chronic Fatigue Syndrome Theory
With the HR stuck in the low 50s in the 4/2000 study, I think the "autonomic activation" model is going to be a hard-sell.
Muffy
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Re: The Saga of SLJ: 40 Years In The Desert
I'm thinking standard autonomic-activation modeling just may turn out to be slightly misleading here. A nonpathological system model of heightened autonomic activation applies with slight or no modification to common pathological autonomic activation.
I would consider the possibility that extended periods of hypothetical phenotype or trait heightened-cognitive arousability, just may allow for intermittent periods of paradoxical or otherwise short-term atypical CNS responses. I would think correlative concomitant-disorder data in epidemiology can help to reject or support this theory.
The most striking common pathology between CFS and CompSAS/CSDB patients: that following-day fatigue that is grotesquely disproportionate with residual AHI for those CompSAS/CSDB patients. I would thus wonder how daytime arousabilty traits compare in those two populations alone. And I would wonder how the wake-to-sleep transition compares---as well as the remainder of sleep in relation to cortical/autonomic arousals.
I would consider the possibility that extended periods of hypothetical phenotype or trait heightened-cognitive arousability, just may allow for intermittent periods of paradoxical or otherwise short-term atypical CNS responses. I would think correlative concomitant-disorder data in epidemiology can help to reject or support this theory.
The most striking common pathology between CFS and CompSAS/CSDB patients: that following-day fatigue that is grotesquely disproportionate with residual AHI for those CompSAS/CSDB patients. I would thus wonder how daytime arousabilty traits compare in those two populations alone. And I would wonder how the wake-to-sleep transition compares---as well as the remainder of sleep in relation to cortical/autonomic arousals.
-
SaltLakeJan
- Posts: 776
- Joined: Sat Jan 17, 2009 8:49 pm
- Location: Salt Lake City, Utah
Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
Mornin' Muffy,
When I opened the thread this a.m., I was amazed at the analysis you made in such a short time. I have printed it out for detailed reading. Interesting, that you caught my error on Mirapex. At one time, (don't recall when), Costo filled Lyrica and Mirapex at the same time,& listed on the containers 150 mg ea. (The card copy had 1.5) The pills were identically to 1.5 mg I was taking. But the 150 mg stuck in my mind. I have seen my doctors many times since then. Each time they check my list of medications, (Mirapex has been listed at 2, 150 mg tablets. The excessive dose didn't sink into their minds, until the new sleep doctor noticed it. He said it wasn't possible for me to take 300 mg. per day. THE TWO OF YOU WERE THE ONLY ONES TO ABSORB WHAT YOU READ.
I apologize for the error, I do scan each post for accuracy, however trying to keep each post clear & accurate is a real memory challenge. I'D LIKE TO ADD ONE WORD TO YOUR POST TITLE, IT IS THE COMPLEX SAGA OF 40 YEARS IN THE DESERT.
I have an additiional graph for the 9-2001 sleep study. Photobucket refuses to upload it. It was resized with all the others) When I get back today, I'll try another photo site.
I have had sharp pains in tooth #3, The dentist doesn't know if it is the temporary crown, or if root canal is acting up. Today, I will be seeing one, if not two dentists.
I posted that after my 9-2001 sleep test, that my internist decided to specialize. I don't have the time this morning to research the date and amount of Mirapex originally prescribed, but I can find it. My next internist prescribed it at a very low dose. I saw him about 6 month intervals, & he either increased the dose or doubled the pills until I was taking 2, 1.5 mg.
TPKAPFKAS. very clever.
When I opened the thread this a.m., I was amazed at the analysis you made in such a short time. I have printed it out for detailed reading. Interesting, that you caught my error on Mirapex. At one time, (don't recall when), Costo filled Lyrica and Mirapex at the same time,& listed on the containers 150 mg ea. (The card copy had 1.5) The pills were identically to 1.5 mg I was taking. But the 150 mg stuck in my mind. I have seen my doctors many times since then. Each time they check my list of medications, (Mirapex has been listed at 2, 150 mg tablets. The excessive dose didn't sink into their minds, until the new sleep doctor noticed it. He said it wasn't possible for me to take 300 mg. per day. THE TWO OF YOU WERE THE ONLY ONES TO ABSORB WHAT YOU READ.
I apologize for the error, I do scan each post for accuracy, however trying to keep each post clear & accurate is a real memory challenge. I'D LIKE TO ADD ONE WORD TO YOUR POST TITLE, IT IS THE COMPLEX SAGA OF 40 YEARS IN THE DESERT.
I have an additiional graph for the 9-2001 sleep study. Photobucket refuses to upload it. It was resized with all the others) When I get back today, I'll try another photo site.
I have had sharp pains in tooth #3, The dentist doesn't know if it is the temporary crown, or if root canal is acting up. Today, I will be seeing one, if not two dentists.
I posted that after my 9-2001 sleep test, that my internist decided to specialize. I don't have the time this morning to research the date and amount of Mirapex originally prescribed, but I can find it. My next internist prescribed it at a very low dose. I saw him about 6 month intervals, & he either increased the dose or doubled the pills until I was taking 2, 1.5 mg.
TPKAPFKAS. very clever.
Regard the Chronic Fatigue Syndrome, I have had overwhelming fatigue for years, When I think about it, I have to pesume you can have as many or few symptoms with it , as you have. Re: hyperactive cognition, would that relate to insomnia? When I used to go to bed, so many interesting ideas would occur, that I liked to stay awake and let a thought develop. However, since starting Cpap, the sensation of pressured breathing has kinda a hyponotic effect. It still takes a while for me to fall asleep. That may be long term habitual behavior. I have less than a month before my sleep study. I am starting an earlier bed time, perhaps this will help me get a longer sleep time in the study. I can't find the words I want to use to thank you, for the time you are spending on the search to discover the source of my problems. JanMuffy wrote:-SWS wrote:
In light of the observations above, and the CFS diagnosis that Jan received, I have some interesting supporting links and pathophysiologic conjecture about hyperactive cognition-based arousals possibly having some degree of interrelatedness in neurology between overlapping CFS pathology and that of CompSAS/CSDB. Also a comment about a possible neurological stimulus/response mechanism that just may exist as an interrelated cohort for this particular hypothetical patient phenotype in neurology.
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Additional Comments: Began CPAP 1-16-2009, Pressure=10 cm, Mask, CMS 50Plus Oximeter |