






The moral of this thread ... everyone is different!
Different people do better with different masks.
Different people do better with different machine brands/models.
Different people do better with different machine settings.
YOU have options.
So find the mask that works best for YOU.
Find the PAP mode (cpap, apap, bi-level) that works best for YOU.
Find the pressure(s) that work best for YOU.
Empower yourself by taking control of your treatment (DMEs, RTs, and docs care more about making a living than YOUR health ... accept this fact), learn of your condition, learn of your options, learn by reading this forum. It takes time for all of this knowledge (from forum posts and your own trial and error) so be patient.
Comparison Resmed S8 AutoSet II vs Remstar M Series
-
DreamStalker

- Posts: 7509
- Joined: Mon Aug 07, 2006 9:58 am
- Location: Nowhere & Everywhere At Once
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
President-pretender, J. Biden, said "the DNC has built the largest voter fraud organization in US history". Too bad they didn’t build the smartest voter fraud organization and got caught.
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
You're so right, DreamStalker!
ozij, thank you for the interesting link:
ozij, thank you for the interesting link:
I hope the researchers thought to keep C-Flex turned off in the "RR" (Respironics REMstar Auto) during the study, to make the comparison as equal as possible in regard to exhalation. I didn't see any mention of that, and I don't recall if C-Flex is "on" by default when a person receives a Respironics Auto. Probably it is "off" by default.ozij wrote:For those interested in an academic comparison of algorithms responding to real patients:
Titration Efficacy of Two Auto-Adjustable Continuous Positive Airway Pressure Devices Using Different Flow Limitation-Based Algorithms
This was published in Respiration, vol. 75 no.1 2008 and is fully downloadable.For those interested in an academic comparison of algorithms responding to real patients:
Titration Efficacy of Two Auto-Adjustable Continuous Positive Airway Pressure Devices Using Different Flow Limitation-Based Algorithms
This was published in Respiration, vol. 75 no.1 2008 and is fully downloadable.
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435

Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
Since machines are relatively expensive and especially since today many are purchasing their machines out of pocket, can't data from sleep studies and titrations be used to help evaluate the likely effectiveness of one algorithm over another? It's much more expensive to try on machines by trial and error than masks!
Say a person is titrated at 14, has numerous apneas (we all know what those are) requiring 14, very little snore or flow limitations.
Wouldn't this information be used to make an equipment determination? Can an educated prediction be made for the likelihood of effective therapy by one machine over the other?
Thanks for your indulgence,
Georgio
Say a person is titrated at 14, has numerous apneas (we all know what those are) requiring 14, very little snore or flow limitations.
Wouldn't this information be used to make an equipment determination? Can an educated prediction be made for the likelihood of effective therapy by one machine over the other?
Thanks for your indulgence,
Georgio
DreamStation 2, Oscar
Resmed AirFit P30i Nasal Mask
Resmed AirFit P30i Nasal Mask

Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
SWS-SWS wrote:Apparently A10's response above 10 cm is sufficiently counterintuitive to lead newcomers and old timers to the wrong conclusion about A10's effectiveness.dsm wrote:I know you were merely repeating what you had been fed repetedly by others who either knew better or should have.
But the answer to clarifying that A10 confusion is not all the name calling and character-condemning accusations that I have been on the receiving end in this thread, Doug. Your protective Resmed policy of: 1) suggesting that there are now brand new pressure responses above 10 cm, and of 2) referring to old-timers such as myself who perfectly understand A10 as if they were exploitative liars is really at the heart of why this thread has repeatedly diverged from rationality starting on page one.
I'll restate what I think the inherent problem really is: A10's statistically-based pressure response above 10 cm is sufficiently counterintuitive to lead newcomers and some old timers to the wrong conclusion about A10's overall effectiveness.
Doug, let's nail it down with rational discussion, but let's not castigate people around here with false character insults about deceptiveness and exploitation.
Lets get it straight. From the beginning I made the point that quoting the A10 mantra or as Georgio did, stating that Resmed doesn't respond to apnea over 10 cms is plainly misleading. This whole thread is littered with evidence of this simple point.
You stepped into the thread & said 'what is wrong with the a10 mantra - it is factual' I then repeated it is misleading you then repeated where is it incorrect etc: etc: etc: etc: etc:
You were sticking to your point that the A10 mantra is a statement of fact & I was sticking my point that started this aspect of the thread, that it is misleading to newcomers and therefore serves no purpose - it is being delivered out of context & thus misleads. From where I sit, you were not dealing with the issue I raised but created your own red herring & for that I consider you have to have known what you were up to. Had there been a meeting of the minds we could have discussed it. It took some newer members to point out that yes the A10 mantra is misleading & a couple then added in qualifications (velbor) that had the effect of putting a better context around the a10 comments.
The other characterizations (yours and mine - implied or blunt) were and are distractions & don't relate to the core point. I must say I am more than disappointed that we could not follow a sensible path together on this issue. I take half the blame for that.
DSM
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
Georgio, if anyone happened to present prolific obstructive apneas at 14 cm----coupled with little flow-limitation and snore signals at 14 cm-----then they'd be very wise to avoid A10.Georgio wrote:Say a person is titrated at 14, has numerous apneas (we all know what those are) requiring 14, very little snore or flow limitations.
Wouldn't this information be used to make an equipment determination?
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
Georgio,Georgio wrote:Since machines are relatively expensive and especially since today many are purchasing their machines out of pocket, can't data from sleep studies and titrations be used to help evaluate the likely effectiveness of one algorithm over another? It's much more expensive to try on machines by trial and error than masks!
Say a person is titrated at 14, has numerous apneas (we all know what those are) requiring 14, very little snore or flow limitations.
Wouldn't this information be used to make an equipment determination? Can an educated prediction be made for the likelihood of effective therapy by one machine over the other?
Thanks for your indulgence,
Georgio
You don't just have an OSA APNEA (the apnea as defined to mean a no-flow ) without some prior closure of the airway. That prior closing off typically happens over time and many breaths - next to no one goes from a normal breath to an APNEA unless they are having a central. That can happen by someone turning over in their sleep. A central following a turnover is very normal - but no snores & little to no flattening.
ADD to this the fact that someone with 10 CMs of pressure already has an air force there trying to keep the airway open. We are NOT dealing with someone who is not on cpap (their OSA is likely to happen quicker without the stenting effect of the 10+ CMs of air).
The normal OSA pattern is for the airway to start collapsing as the muscles relax and this begins with flattening of the insp curve AND OPTIONALLY snores.
That flattening is there for FLs, Hypopneas and APNEAS (as defined by the manufacturers of their machines).
Repeating, OSA tends to develop over minutes which is why Autos take minutes to change their pressure. None do so instantly, they all do so in small increments. The fastest I know of any machine upping pressure in a single step is IIRC the Respironics may do so when a particular SDB pattern is detected. The Resmeds do it in 0.2 increments (I can't recall if they do any 0.5 or 1.0 jumps - the early models may have but the later ones I believe don't).
DSM
#2 just saw SWS's post & yes I agree that there may be exceptions (I doubt many) but they are bound to occur & yes the Respironics algorithm is possibly the better bet should such cases be identified.
Last edited by dsm on Tue Apr 07, 2009 4:11 pm, edited 2 times in total.
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
Thank you SWS, that was my whole point of raising the question in the first place! I don't know what size that segment of OSA patients is, however that information seems very relevant, and useful to us newcomers, when making an equipment investment.
And based on the study cited earlier, and IMHO, if you want to sleep longer, at lower pressures, with faster pressure adjustments and with a lower AHI, one should get a Resperonics anyway.
Georgio
And based on the study cited earlier, and IMHO, if you want to sleep longer, at lower pressures, with faster pressure adjustments and with a lower AHI, one should get a Resperonics anyway.
Georgio
DreamStation 2, Oscar
Resmed AirFit P30i Nasal Mask
Resmed AirFit P30i Nasal Mask
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
Georgio,the OA/FL/snore pattern that you suggest is not a complete rarity IMHO.
But let me add to my statement above by saying that under those somewhat uncommon OA/FL/snore circumstances, I would also avoid the Respironics algorithm and just run a BiLevel or CPAP:
But let me add to my statement above by saying that under those somewhat uncommon OA/FL/snore circumstances, I would also avoid the Respironics algorithm and just run a BiLevel or CPAP:
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
SWS,
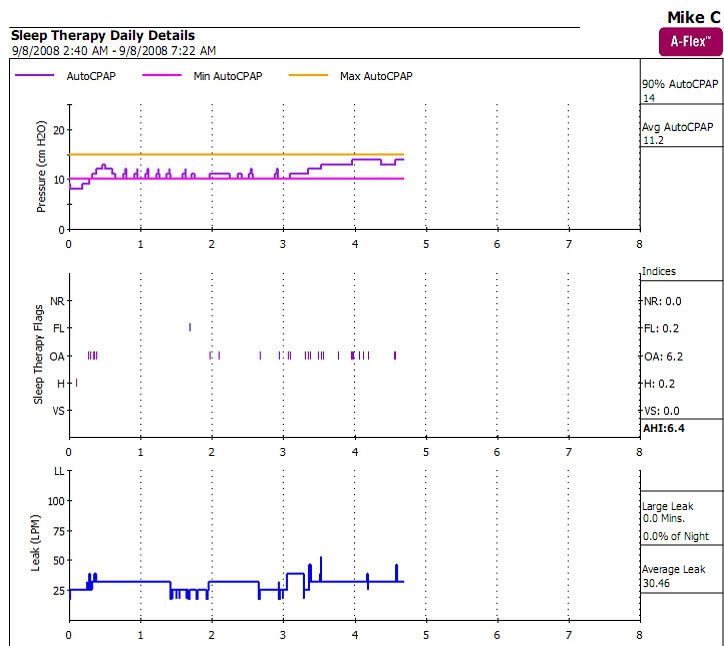
Thanks for posting that chart, it is helpful for me to point out the characteristic 'chairs' that represent the way Respironics machines probe with a pattern of pressure variations.
That is what the Resmed doesn't do. It monitors the flattening of the INSP curve breath-by-breath & will adjust pressure if it determines the flattening is leading to a hypopnea or APNEA.
DSM
Thanks for posting that chart, it is helpful for me to point out the characteristic 'chairs' that represent the way Respironics machines probe with a pattern of pressure variations.
That is what the Resmed doesn't do. It monitors the flattening of the INSP curve breath-by-breath & will adjust pressure if it determines the flattening is leading to a hypopnea or APNEA.
DSM
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
-
rested gal
- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
Since neither of the two major brands of autopaps (Respironics and ResMed) treat a sudden apnea, I doubt if that kind of information would be useful for choosing between one brand or the other.Georgio wrote:Since machines are relatively expensive and especially since today many are purchasing their machines out of pocket, can't data from sleep studies and titrations be used to help evaluate the likely effectiveness of one algorithm over another? It's much more expensive to try on machines by trial and error than masks!
Say a person is titrated at 14, has numerous apneas (we all know what those are) requiring 14, very little snore or flow limitations.
Wouldn't this information be used to make an equipment determination? Can an educated prediction be made for the likelihood of effective therapy by one machine over the other?
Thanks for your indulgence,
Georgio
Information from a sleep study about that kind of scenario (a sudden apnea scenario that's probably rather unusual, imho) would be more useful in making a decision where to set the minimum pressure in the range when using either brand, I'd think. But not so much so in the choice of brand.
However, if no one person in the "what settings shall we use for the autopap" loop is very savvy about the importance of putting the minimum pressure setting up quite close to 14 in that scenario... not the doctor, the DME, an RT, or the end user himself/herself... then possibly a Respironics machine might be the better choice. For that unusual scenario.
The Respironics machine would at least try a few increased pressure nudges to see if more pressure showed any improvement in the air flow. Maybe a small increase or two during the "nudging" would improve the situation. But most likely not, imho, since without flow limitations already moving the pressure up, the machine would probably be operating at such a low pressure that a few increase nudges probably wouldn't change the situation and the Respironics machine would then do just like the ResMed machine -- wait for the apnea to clear on its own, i.e, the person arouse enough to take another breath.
I don't think that kind of sudden apneas scenario (or the hope that a pressure nudge or two would improve things) are likely enough to warrant choosing one brand over the other.
That kind of "known" scenario (if actually "known") would be good reason, however, imho, to set the minimum pressure up near, or on, 14 right from the get-go. If a person wanted exhalation relief, that kind of scenario might be good reason to think about setting a higher minimum pressure (15 or 16) if a person were going to use EPR with a ResMed machine, or stick with 14 for the minimum and choose Respironics' A-Flex.
Or...just use any brand of CPAP at 14.
Last edited by rested gal on Tue Apr 07, 2009 4:23 pm, edited 1 time in total.
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435

Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
How many sleep-deprived patients, sleep doctors or DMEs are going to do that? (he said, with tongue-in-cheek)Georgio wrote:Since machines are relatively expensive and especially since today many are purchasing their machines out of pocket, can't data from sleep studies and titrations be used to help evaluate the likely effectiveness of one algorithm over another? It's much more expensive to try on machines by trial and error than masks!
Say a person is titrated at 14, has numerous apneas (we all know what those are) requiring 14, very little snore or flow limitations.
Wouldn't this information be used to make an equipment determination? Can an educated prediction be made for the likelihood of effective therapy by one machine over the other?
Thanks for your indulgence,
Georgio
One of the bigger argumentative threads I remember on the forum occurred when it was suggested by "someone" (not me and I'm not mentioning any names) that patients be able to try a number of different machines before getting the one that worked best for them.
Most of the time, patients don't even have the awareness that there are data-capable machines or even have a choice of what's handed to them. Most of the DMEs only carry Respironics or ResMed (or MAYBE Fisher & Paykel). They usually get whatever makes the most money for the DME. How would you determine which machine worked the "best" for you? You'd also have to have the software that went with that machine.
Pretty expensive proposition to evaluate what works for you.
Den
(5) REMstar Autos w/C-Flex & (6) REMstar Pro 2 CPAPs w/C-Flex - Pressure Setting = 14 cm.
"Passover" Humidification - ResMed Ultra Mirage FF - Encore Pro w/Card Reader & MyEncore software - Chiroflow pillow
User since 05/14/05
"Passover" Humidification - ResMed Ultra Mirage FF - Encore Pro w/Card Reader & MyEncore software - Chiroflow pillow
User since 05/14/05
-
rested gal
- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
Right. That's why I went back and edited mine to add -- (if actually "known")Wulfman wrote:How many sleep-deprived patients, sleep doctors or DMEs are going to do that? (he said, with tongue-in-cheek)
Wasn't me either. I remember that.Wulfman wrote:One of the bigger argumentative threads I remember on the forum occurred when it was suggested by "someone" (not me and I'm not mentioning any names) that patients be able to try a number of different machines before getting the one that worked best for them.
Last edited by rested gal on Tue Apr 07, 2009 4:28 pm, edited 1 time in total.
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
Rested Galrested gal wrote:Since neither of the two major brands of autopaps (Respironics and ResMed) treat a sudden apnea, I doubt if that kind of information would be useful for choosing between one brand or the other.Georgio wrote:Since machines are relatively expensive and especially since today many are purchasing their machines out of pocket, can't data from sleep studies and titrations be used to help evaluate the likely effectiveness of one algorithm over another? It's much more expensive to try on machines by trial and error than masks!
Say a person is titrated at 14, has numerous apneas (we all know what those are) requiring 14, very little snore or flow limitations.
Wouldn't this information be used to make an equipment determination? Can an educated prediction be made for the likelihood of effective therapy by one machine over the other?
Thanks for your indulgence,
Georgio
Information from a sleep study about that kind of scenario (a sudden apnea scenario that's probably rather unusual, imho) would be more useful in making a decision where to set the minimum pressure in the range when using either brand, I'd think. But not so much so in the choice of brand.
However, if no one person in the "what settings shall we use for the autopap" loop is very savvy about the importance of putting the minimum pressure setting up quite close to 14 in that scenario... not the doctor, the DME, an RT, or the end user himself/herself... then possibly a Respironics machine might be the better choice. For that unusual scenario.
The Respironics machine would at least try a few increased pressure nudges to see if more pressure showed any improvement in the air flow. Maybe a small increase or two during the "nudging" would improve the situation. But most likely not, imho, since without flow limitations already moving the pressure up, the machine would probably be operating at such a low pressure that a few increase nudges probably wouldn't change the situation and the Respironics machine would then do just like the ResMed machine -- wait for the apnea to clear on its own, i.e, the person arouse enough to take another breath.
I don't think that kind of sudden apneas scenario (or the hope that a pressure nudge or two would improve things) are likely enough to warrant choosing one brand over the other.
That kind of "known" scenario (if actually "known") would be good reason, however, imho, to set the minimum pressure up near, or on, 14 right from the get-go. If a person wanted exhalation relief, that kind of scenario might be good reason to think about setting a higher minimum pressure (15 or 16) if a person were going to use EPR with a ResMed machine, or stick with 14 for the minimum and choose Respironics' A-Flex.
Or...just use any brand of CPAP at 14.
Very well said - very clear - sure works for me
Cheers
DSM
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
KEY points those. And that is EXACTLY why that the tired repeating of the "don't buy a ResMed auto if you want a machine that responds to apneas that occur above 10 cm" mantra is misleading to the point of being ignorant falsehood in the context in which it is so often trotted out. If NEITHER brand "treats" the lone frank sudden apnea scenario, why is it so often stated by some in such an oversimplified way as to imply one brand does and the other doesn't? Sure, one brand may claim to "respond" and another brand may claim to "prevent." Sure, the algorithms are imperfect and have overall approaches that differ. But when someone comes to this forum to ask what brand to buy, what purpose does it serve to point out limitations of one brand's auto algorithm without giving equal time to the other brand's algorithm limitations? Newbies aren't hearing "I prefer this brand," when that is stated; they are hearing "that brand is flawed." I think it is only because someone thinks he understands the limits of one, but doesn't grasp the limits of the other, that such a statement keeps being made to newbies. And the statement is made repeatedly in that very context. So, yes, I am one of the ones irritated by it, just like DSM.rested gal wrote: . . . neither of the two major brands of autopaps (Respironics and ResMed) treat a sudden apnea . . .
. . . I don't think that kind of sudden apneas scenario . . . [is] . . . likely enough to warrant choosing one brand over the other.
-SWS sums up the problem beautifully with the common repetitions of the A10 statement when he says:
So, then, why should anyone repeatedly state something counterintuitive to new ones, without explanation, to them, when it is much more likely to lead to wrong conclusions than it is to be actual helpful information? -SWS doesn't do that, and I don't think others should do it either, in my opinion. When a newbie asks "what machine should I get" and the answer implied is that ResMeds are somehow grossly ineffective because of their algorithm, I have to agree with DSM that the statement is damagingly misleading. The problem with oversimplifying the algorithm differences is that doing so, it seems to me, so often obscures the infinitely more important facts newbies considering autos need to know. They need to know that they can use the data to tweak therapy regardless of brand. And they need to know that, whichever auto they buy, they may end up having to set the minimum on the auto close to, or maybe even at, their prescribed pressure, for effective therapy, if they choose to continue to run it in auto mode. The message needs to be "all brands of autos are flawed," not "one brand of autos is flawed," if, in fact, flaws are what need to be addressed in the discussion.-SWS wrote:I'll restate what I think the inherent problem really is: A10's statistically-based pressure response above 10 cm is sufficiently counterintuitive to lead newcomers and some old timers to the wrong conclusion about A10's overall effectiveness.
So, why don't we give the useful information to the newbies, instead of repeatedly confusing them by implying one machine is hands-down more effective than the other? After all, when people come here looking to buy a machine, they aren't interested in hypotheticals and rare scenarios. They want to know what works. And the answer is: NO auto works perfectly, so whichever one you buy, you will need to look at your data and set your minimum and maximum according to what YOU will need. Here are some feature differences, etc . . .
On a side note: SAG, you strike me as a highly-educated, talented, brilliant man. So I think I understand part of your reasons for your heartfelt disdain that so much misinformation (and disinformation) gets preserved in some threads on this board at times. But my concern is this: If a newbie were to come here today and read your name-calling (warranted or not, jokingly said or not), that newbie might not take your other posts as seriously as he or she should. Indeed, that CPAP-newbie, if not a forum-user-newbie, might even decide to put you on his or her enemies list. And that would be a true shame, because your contribution here is particularly valuable to all of us. Personally, that thought worries me much more than anything else I've read in this thread. I hope you don't mind me saying so. Your reputation matters to me.
jeff
Re: Comparison Resmed S8 AutoSet II vs Remstar M Series
JNK,
That is an impressive post and sums up so much of what needs to be addressed.
Also your comment re SAG, I too do value his expertise. What got brought up in his regard is what can be called self-inflicted wounds. I hope he is big enough to let it pass & show he can interact with people he might disagree with or may not even like. All the mature people here seem to keep dialogues open even when perhaps not wanting to. We are a diverse group & there will always be niggles. Sometimes those niggles breakthrough & we get 'narky' with each other. I am guilty of letting my frustrations show & apologize for that. I do try to make up for it by always giving praise & support where it is earned and to people I have been in disagreement with.
Your post confirms my faith that there can be a meeting of the minds even if preceded by pointed disagreement.
Cpaptalk at it best.
DSM
That is an impressive post and sums up so much of what needs to be addressed.
Also your comment re SAG, I too do value his expertise. What got brought up in his regard is what can be called self-inflicted wounds. I hope he is big enough to let it pass & show he can interact with people he might disagree with or may not even like. All the mature people here seem to keep dialogues open even when perhaps not wanting to. We are a diverse group & there will always be niggles. Sometimes those niggles breakthrough & we get 'narky' with each other. I am guilty of letting my frustrations show & apologize for that. I do try to make up for it by always giving praise & support where it is earned and to people I have been in disagreement with.
Your post confirms my faith that there can be a meeting of the minds even if preceded by pointed disagreement.
Cpaptalk at it best.
DSM
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)