BTW, the missing nights are either because I forgot to put the card in or, recently, because I was using a different machine and the Analyzer program doesn't work with the SV. I have been 100% compliant since day one.
Bev
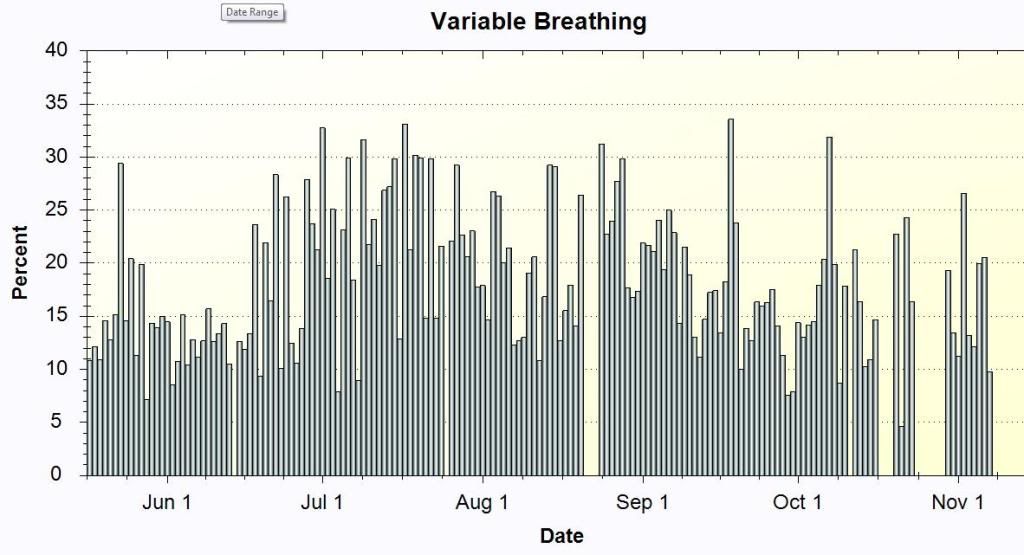
StillAnotherGuest wrote:-SWS wrote:Don't know about Lexapro, but I think this may be the only variable breathing chart that Bev ever posted. Wonder if her VB was more pronounced during Lexapro use. This isn't much VB compared to Browser's:
<snipped: Bev's VB chart shown one post above>
But according to the "SAG Interpretive Guide To Variable Breathing Percentages" (which he made up), she'd still have periods that were markedly abnormal:
Code: Select all
< 5.0% Normal 5 - 15% Mild Disturbance 15 - 25% Moderate Disturbance > 25% Severe DisturbanceNo, because I believe it would be "the other channels" where all the significant events would be occurring (wake, where respiratory events are not scored, phasic REM, where that type of breathing should be appreciated as normal phenomena, and if I understand the VB concept correctly, this variability is often "breath-to-breath", or nearly so, with normal "breaths" (other than variation in peak flow, seen as changes in amplitude w/o a plateau effect), so there wouldn't be anything that could be called a "respiratory event" per se.ozij wrote:SAG - is there an equivalent to "variable breathing" in a real life PSG? I mean, do you ever look at a PSG and say "Gee, that there is <insert variable breathing equivalent> - wonder what's going on in other channels?"
Yeah, given the Entry Qualifications for that poll, I don't see where there'll be a lot of takers.-SWS wrote:I just placed a VB poll with open discussion here:
viewtopic/t36541/Encore-Analyzer-Variab ... -Poll.html
Would love to find more out about this topic. So would Browser and others I'll bet!
But if anybody who doesn't have EPA wants to know their VB%, export their Encore file to desktop, open up the *.xml file with IE, do a search for "variable" and you'll find it.
I would not dismiss the significance of high-to-very high VB% under any circumstances. I firmly believe that either severe sleep architectural disturbances exist and/or the treatment algorithm has been suspended (of course, given how the VB Controller works, the latter would be a good thing)(except maybe if you woke up and the pressure was pegged).ozij wrote:(VB) was pulled out of the dark hole in the SQL database not meant for either clincians or patients by, message board users trying create a better presentation of their results than Encore

Snoredog, does that translate to an VB trends that you've noticed?Snoredog wrote:So for me it's one night of good sleep and two awake. While I try to avoid them, if I watch TV I get bored and will nap,
then I start in with those onset events, hyperventilating over and over feeling really uneasy, where I have to get up go outside or do something else to stop it.
I have 2 machines an Aflex and 420e, I'll use one for a while get in a rut, then switch to the other and back and forth.
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |

And I put it in EPA because Derek had it in MyEcnoreWulfman wrote:I remember back when we had these similar conversations with Derek (when he brought out MyEncore). He said it was in the database so he put it into his program.
Your not alone... I always have tended to have a VB in that range also.Browser wrote:I am the only person who voted 50-60% so far..
James, were you ever able to correlate your VB to one more than the other: 1) your CSDB, 2) your extreme nasal and airway impedance problems, 3) other?jskinner wrote:I always have tended to have a high VB value. Typically between 50-60%
Might be a good candidate for the autoSV, Snoredog.So for me it's one night of good sleep and two awake. While I try to avoid them, if I watch TV I get bored and will nap,
then I start in with those onset events, hyperventilating over and over feeling really uneasy, where I have to get up go outside or do something else to stop it.
I have 2 machines an Aflex and 420e, I'll use one for a while get in a rut, then switch to the other and back and forth.
Maybe you haven't checked enough mountains......-SWS wrote:James, were you ever able to correlate your VB to one more than the other: 1) your CSDB, 2) your extreme nasal and airway impedance problems, 3) other?jskinner wrote:I always have tended to have a high VB value. Typically between 50-60%
Ozij, I was going to make a funny comment about your helicopter post... but the helicopter took off! Also, I need to come clean that there are no hotdog stands at the top of that mountain.
Also, I'd like to link to a relevant side discussion between georgepds and dsm:
viewtopic.php?f=1&t=36442&start=45#p316526
Breashear's book read with Krakauer's "Into Thin Air" are a thought provoking combination.The next day, while Breashears stayed at Camp 3 to assist descending climbers, Schauer and Viesturs hiked to Camp 4 to help bring Weathers down. For most of the morning, the Texan was half-led, half-carried down the slope, at one point sitting still while he was secured with rope and lowered like a 200-lb. rucksack. When the team reached Camp 3, they were joined by Breashears and a group of Sherpas bringing Makalu Gao down. Together they trekked to Camp 2, where they learned that a helicopter--which could never have stayed aloft in the tenuous air near the top of the mountain--would now be able to meet them and evacuate the wounded. Before long, the climbers heard the whap-whapping of blades and saw a dark green chopper struggling up to them. When it landed, the able-bodied loaded first Makalu Gao, then Weathers aboard, and the pilot flew off, dropping gratefully down to lower altitudes where there was thicker air for his blades to bite. With the helicopter gone, the most grievously injured climbers were at last on their way to safety. Back on Everest, the ambulatory ones were left to make their own way down--and the fallen ones were left to remain forever where they lay.
I swear I'm using not the Mallory quote to hint at the usefulness or otherwise of the VB statistic.....The first question which you will ask and which I must try to answer is this; What is the use of climbing Mount Everest? and my answer must at once be, it is no use. There is not the slightest prospect of any gain whatsoever.
George Leigh Mallory
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
Yeah, I guess that doesn't make much sense without the deleted post or some background to go by. Ozij had humorously and correctly mentioned that helicopters can't make it to the top of the highest-altitude mountains. Those would be the mountains without the picnic tables and hot dog stands up top.Wulfman wrote:-SWS wrote:Ozij, I was going to make a funny comment about your helicopter post... but the helicopter took off! Also, I need to come clean that there are no hotdog stands at the top of that mountain.
Maybe you haven't checked enough mountains......
There are lots more mountains out here. Maybe you'd better come out and check them before ruling out hotdog stands being on mountain tops.
Den (thinking that strange posts deserve equally strange responses)
I just spotted the comment about the high 40's, Den. Thanks for adding that early on.Wulfman wrote:... my range has been from about 20 to the high 40's (those are very rare) with the typical night being somewhere between 25 and 35. And, remember......my pressure is fixed at 12.
At this point I'm thinking your experience might be somewhat typical. Perhaps VB variability is to be expected---and perhaps nothing is wrong with sleep or health unless VB gets inordinately high. My hunch is that if VB gets very high, then something may be very wrong with sleep and/or health.Wulfman wrote:I've tried to correlate it with AHI......can't do it. I had an AHI of 0.0 last night and my VBF was right at 30.....I had a 0.1 the night before and my VBF was about 20......and I've had good and bad nights (in terms of sleep quality and AHI) with similar and different VBF numbers.
I've sure vacillated back and forth regarding this clue as well. My take is that the entire SQL data set was designed for APAP. Then a year or two later that APAP machine with SQL data set served as the foundation for the very first data-capable CPAP machine. A cost-effective design approach would be to just stub off the APAP treatment algorithms, but not the detection algorithms to make that data-capable CPAP.Wulfman wrote:I've wondered if it has something to do with the REMstar Auto's algorithm, but then it's also being logged in the data-capable CPAP machines.