







Oh, thank goodness, I thought he was thinking that I had CHF (I googled it so I know what that means).
Here's an example of my memory problems, and no, it's not that I'm getting old. At noon, today, I put my Lean Cuisine in the microwave to heat for lunch. Then someone came in unexpectedly that I had to meet with, followed by someone else and then a third person. At 2:30 as I was putting away a file, I felt faint. I went to make a cup of tea and saw the Lena Cuisine box on the ocunter. I thought, "Is this mine? I usally throw them away as soon as I finish cooking." Then I thought, " I don't remember eating this, I must be losing my memory". Then I opened the microwave and there it was, 2 and a half hours later.
Good thing I have that GPS, so I can find my way home!
Bev
Why doesn't APAP respond to apneas?
Re: Why doesn't APAP respond to apneas?
Diagnosed 9/4/07
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1

Re: Why doesn't APAP respond to apneas?
SAG,
I have extracted your comments on Variable Breathing and added them to a thread on the topic that was started some weeks back.
viewtopic/t35402/What-are-Flow-Limitati ... thing.html
That thread also has a helpful extract from the Respironics patent for their AUTO and how it deals with VB. I have also updated that
particular post with the following added para - if this is not accurate please feel free to comment.
*************************
#3 Just adding as a summary, the main way this patent describes how it corrects 'Variable Breathing' is mentioned in paras 177 & 178 & one para says that if pressure has been rising (due to other events) and VB occurs, the machines will start to lower pressure in 0.5 CMs increments & the other action occurs when pressure was going down and VB is detected, then the machine will start raising pressure in 0.5 increments - it seems CMs will go down or up depending what was happening prior to VB being detected.
#4 Variable Breathing is 'erratic' breathing - that is, the person's rate and volume fluctuates erratically. This is different to 'Periodic Breathing' which is usually defined as 'cyclic' changes to volume - Cheynes-Stokes Respiration is a classic form of 'Periodic Breathing'. The sleeper's airflow volume steadily grows over a few minutes (waxes) then drops steadily for a few minutes (wanes) in a 'cyclic' fashion - a pattern of waxing & waning. Cheynes-Stokes is associated with CHF (Congestivec Heart Failure (tks RG)).
*************************
Your definition and divisions of effect are an excellent starting point.
DSM
I have extracted your comments on Variable Breathing and added them to a thread on the topic that was started some weeks back.
viewtopic/t35402/What-are-Flow-Limitati ... thing.html
That thread also has a helpful extract from the Respironics patent for their AUTO and how it deals with VB. I have also updated that
particular post with the following added para - if this is not accurate please feel free to comment.
*************************
#3 Just adding as a summary, the main way this patent describes how it corrects 'Variable Breathing' is mentioned in paras 177 & 178 & one para says that if pressure has been rising (due to other events) and VB occurs, the machines will start to lower pressure in 0.5 CMs increments & the other action occurs when pressure was going down and VB is detected, then the machine will start raising pressure in 0.5 increments - it seems CMs will go down or up depending what was happening prior to VB being detected.
#4 Variable Breathing is 'erratic' breathing - that is, the person's rate and volume fluctuates erratically. This is different to 'Periodic Breathing' which is usually defined as 'cyclic' changes to volume - Cheynes-Stokes Respiration is a classic form of 'Periodic Breathing'. The sleeper's airflow volume steadily grows over a few minutes (waxes) then drops steadily for a few minutes (wanes) in a 'cyclic' fashion - a pattern of waxing & waning. Cheynes-Stokes is associated with CHF (Congestivec Heart Failure (tks RG)).
*************************
Your definition and divisions of effect are an excellent starting point.
DSM
Last edited by dsm on Thu Nov 06, 2008 12:19 am, edited 1 time in total.
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
Re: Why doesn't APAP respond to apneas?
I just submitted a question about periodic breathing into the above link.
-
rested gal

- Posts: 12881
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
Re: Why doesn't APAP respond to apneas?
Just for clarification.... I think CHF means "Congestive (not "Chronic") Heart Failure."dsm wrote:Cheynes-Stokes is associated with CHF (Chronic Heart Failure).
http://www.americanheart.org/presenter. ... ifier=4585
Yes, Cheyne-Stokes Respiration is often associated with CHF.
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Re: Why doesn't APAP respond to apneas?
Tks RG - will fixrested gal wrote:Just for clarification.... I think CHF means "Congestive (not "Chronic") Heart Failure."dsm wrote:Cheynes-Stokes is associated with CHF (Chronic Heart Failure).
http://www.americanheart.org/presenter. ... ifier=4585
Doug
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
-
StillAnotherGuest

- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
In Summary...
OK, this'll fit on a rubber band (if you write small):OutaSync wrote:I think that I will be able to go back to find the information, but this thread is so long. I've taken pages of notes and printed out pages, trying to re-read and understand. Y'all confuse me, and believe me, it's not hard to do.
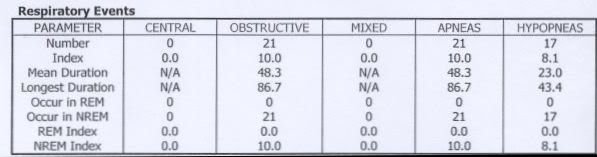
The (albeit brief and incomplete) diagnostic portion of the study says you're plain ol' obstructive:
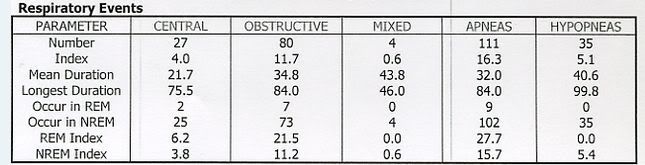
Dysregulation appears with the application of pressure:
I don't see any reason to doubt the data of the M-Series which indicates your SDB is stable.
The AHI on CPAP 14.0 cmH2O is 1.4.
Circulation time does not indicate any cardiac flow problems that would contribute to SDB.
The Ambien Effect is extremely powerful, makes you two different people and dial wingin' very dangerous.
The amount of EDS cannot be explained by the available SBD data presented.
The amount of EDS cannot be explained by the available sleep architecture data presented.
Insert new NPSG and MSLT results here (use additional rubber band if necessary):
SAG

Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.

Re: Why doesn't APAP respond to apneas?
I think you have to conclude with AHI consistently at 2 or less, that the mean avg. includes BOTH obstructive and central phenotypes, this is much lower than seen on the NPSG. At the 14 to 17 cm range on AFLEX there are no NRAH flags being presented so you have to conclude that the PB and Central dysregulation are well under control with that therapy.
With all things considered the M Series AFLEX does a very good job for Bev, no extra relief can be expected from the SV or Bilevel that I can see. If her insurance covers it a PSG would be nice to confirm there is no macroarousals contributing to the EDS and the only place you will find that out is in the lab. Since the NPSG above shows fewer CA's in REM and other study the lack of REM, I would continue with the Melatonin hopefully that will encourage more REM.
SAG: any suggestions for Bev in getting past those onset events when she tries to fall asleep?
Because her pressure is up there, I would try setting up a Auto:Ramp to make it easier to fight the insomnia, AFLEX will bypass that if it sees events it needs to address.
Too bad she couldn't rent a Sandman Auto for a week.
With all things considered the M Series AFLEX does a very good job for Bev, no extra relief can be expected from the SV or Bilevel that I can see. If her insurance covers it a PSG would be nice to confirm there is no macroarousals contributing to the EDS and the only place you will find that out is in the lab. Since the NPSG above shows fewer CA's in REM and other study the lack of REM, I would continue with the Melatonin hopefully that will encourage more REM.
SAG: any suggestions for Bev in getting past those onset events when she tries to fall asleep?
Because her pressure is up there, I would try setting up a Auto:Ramp to make it easier to fight the insomnia, AFLEX will bypass that if it sees events it needs to address.
Too bad she couldn't rent a Sandman Auto for a week.
someday science will catch up to what I'm saying...
Re: Why doesn't APAP respond to apneas?
I guess that pretty well sums up where this as got to.
SV PS isn't the answer to Bev's challenges. Her existing AUTO is going to offer a working solution.
DSM
SV PS isn't the answer to Bev's challenges. Her existing AUTO is going to offer a working solution.
DSM
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
Re: Why doesn't APAP respond to apneas?
My comment above wasn't to infer Bev has CHF, but it is always a good idea to know what the signs of it are.rested gal wrote:Just for clarification.... I think CHF means "Congestive (not "Chronic") Heart Failure."dsm wrote:Cheynes-Stokes is associated with CHF (Chronic Heart Failure).
http://www.americanheart.org/presenter. ... ifier=4585
Yes, Cheyne-Stokes Respiration is often associated with CHF.
Below text is from RG's link and reason I mentioned CHF:
The point of the above is the person may be fine during the day but when they go to lay down the edema from the fluids can cause problems with breathing. This shortness of breath while lying flat can show up as variable, periodic and/or hyperventilation.The "failing" heart keeps working but not as efficiently as it should. People with heart failure can't exert themselves because they become short of breath and tired.
As blood flow out of the heart slows, blood returning to the heart through the veins backs up, causing congestion in the tissues. Often swelling (edema) results. Most often there's swelling in the legs and ankles, but it can happen in other parts of the body, too. Sometimes fluid collects in the lungs and interferes with breathing, causing shortness of breath, especially when a person is lying down.
Heart failure also affects the kidneys' ability to dispose of sodium and water. The retained water increases the edema.
How do you diagnose and treat congestive heart failure?
Your doctor is the best person to make the diagnosis. The most common signs of congestive heart failure are swollen legs or ankles or difficulty breathing. Another symptom is weight gain when fluid builds up.
someday science will catch up to what I'm saying...

Re: Why doesn't APAP respond to apneas?
AVAPSSnoredog wrote: With all things considered the M Series AFLEX does a very good job for Bev, no extra relief can be expected from the SV or Bilevel that I can see.
AVAPS: PC AVAPS, EPAP 15, IPAP Min 19, IPAP Max 25, Vt 520ml, BPM 10, Ti 1.8sec, RT 2 (Garage)
BiPAP Auto SV: EPAP 9, IPAP Min 14, IPAP Max 25, BPM 10, Ti 2sec, RT 2 (Travel Machine)
VPAP Adapt SV: EEP 10.4, Min PS 4.4 (Every Day)
Mask: Quattro
BiPAP Auto SV: EPAP 9, IPAP Min 14, IPAP Max 25, BPM 10, Ti 2sec, RT 2 (Travel Machine)
VPAP Adapt SV: EEP 10.4, Min PS 4.4 (Every Day)
Mask: Quattro
Re: Why doesn't APAP respond to apneas?
WHAT would you be trying to fix?Banned wrote:AVAPSSnoredog wrote: With all things considered the M Series AFLEX does a very good job for Bev, no extra relief can be expected from the SV or Bilevel that I can see.
someday science will catch up to what I'm saying...
Re: Why doesn't APAP respond to apneas?
More Tv time.Snoredog wrote: WHAT would you be trying to fix?
AVAPS: PC AVAPS, EPAP 15, IPAP Min 19, IPAP Max 25, Vt 520ml, BPM 10, Ti 1.8sec, RT 2 (Garage)
BiPAP Auto SV: EPAP 9, IPAP Min 14, IPAP Max 25, BPM 10, Ti 2sec, RT 2 (Travel Machine)
VPAP Adapt SV: EEP 10.4, Min PS 4.4 (Every Day)
Mask: Quattro
BiPAP Auto SV: EPAP 9, IPAP Min 14, IPAP Max 25, BPM 10, Ti 2sec, RT 2 (Travel Machine)
VPAP Adapt SV: EEP 10.4, Min PS 4.4 (Every Day)
Mask: Quattro
Re: Why doesn't APAP respond to apneas?
Well, if the Auto is giving me good treatment, then I would have give it up altogether, as I feel no better using it than I did using nothing. Why in the world would I want to tape and strap up the rest of my life just so that I can have more disturbances in my sleep than before?
I've put 14 months of my life into making this work, but you all have convinced me that it isn't going to get any better, no matter what machine I use. This is as good as it gets. Thanks, all...I'll take it from here.
Bev
I've put 14 months of my life into making this work, but you all have convinced me that it isn't going to get any better, no matter what machine I use. This is as good as it gets. Thanks, all...I'll take it from here.
Bev
Diagnosed 9/4/07
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1

Re: Why doesn't APAP respond to apneas?
Bev, this sounds like you're giving up on finding a solution, and I can certainly understand why you'd feel that way. It also sounds like you're not going to continue with your therapy, and that of course is your choice. Much of me wants to scream, "DON'T GO, BEV!!! AND PLEASE DON'T QUIT!!" .... but I won't. We all have to find our own paths in life.
Just a couple of questions....
Are you sure that a solution can't be found? And even though I've read all of these pages, as I've said before, I haven't understood all of them, so I could be completely off base with this: In spite of all of this, aren't you at least getting better oxygenation? If it's ANY better by using your machine, you have to be better off physically than if you don't use it, even if you don't feel like jumping over tall buildings.
I'm still chasing after that "feeling good" milepost, as well. Much empathy.
Marsha
(Don't go, Bev! And please don't quit! )
Just a couple of questions....
Are you sure that a solution can't be found? And even though I've read all of these pages, as I've said before, I haven't understood all of them, so I could be completely off base with this: In spite of all of this, aren't you at least getting better oxygenation? If it's ANY better by using your machine, you have to be better off physically than if you don't use it, even if you don't feel like jumping over tall buildings.
I'm still chasing after that "feeling good" milepost, as well. Much empathy.
Marsha
(Don't go, Bev! And please don't quit! )
Resp. Pro M Series CPAP @ 12 cm, 0 C-Flex, 0 HH & Opus 360 mask (backup: Hybrid) since 8/11/08; member since 7/23/08
A good laugh and a long sleep are the best cures in the doctor's book. ~ Irish Proverb
A good laugh and a long sleep are the best cures in the doctor's book. ~ Irish Proverb
Re: Why doesn't APAP respond to apneas?
I was going to ask you that, how do you feel with no therapy at all?OutaSync wrote:Well, if the Auto is giving me good treatment, then I would have give it up altogether, as I feel no better using it than I did using nothing. Why in the world would I want to tape and strap up the rest of my life just so that I can have more disturbances in my sleep than before?
I've put 14 months of my life into making this work, but you all have convinced me that it isn't going to get any better, no matter what machine I use. This is as good as it gets. Thanks, all...I'll take it from here.
Bev
The thing dangerous about doing that is your oxygen levels drop dangerously low from the PSG from the very long duration of events seen. You cannot allow that to continue. While you don't feel any better due to daytime fatigue the lack of oxygen will destroy
your organs and create even more problems. Lack of memory is one indicator that is happening.
You must stay on a machine or go with supplemental oxygen.
I still think they missed your titration.
My suggestions:
1. I would put the SV back on auction, obviously it is no panacea in your case. If SAG said he didn't see any microarousals possibly
contributing to the daytime fatigue then the SV isn't going to help.
2. I would invest in a decent pulse oximeter like the CMS-50 and software (I can tell you how to install the software on Vista in Windows compatible mode).
3. AFLEX: Put it in CPAP mode w/Cflex at 9.0 cm pressure. While you would still get data, you have to assume what you are looking
at is central events and the machine shouldn't be responding anyway. You had ZERO events on the SV in CPAP mode.
4. Get a Sandman Auto and software (when you sell your other equipment). I'd sell the SV first, get a Sandman Auto with proceeds, sell the Aflex when you can as it is no better for you than the SV was (well a little better but it is the result that counts).
5. Address any allergies (even if you don't think you have any), most of us do.
Allergies: IF you have allergies and are taking something for it, maybe you need to shift when you take them? Such as taking them before bed as opposed to in the morning. Most allergy medications make you drowsy, in fact that is how many of the sleep medications were found to work, fatigue from adverse side effects when using them for allergies. I many times take Loratadine 10mg, before bed if I'm congested, it helps, they say it doesn't make you drowsy but they all do including Zyratec. I buy generic OTC AllerClear at Costco for $15 bucks for 300 tablets, its the same chemical makeup as Claritin only it costs way less. I would avoid the "D" or decongestant type it will overly dry you out, I only use the antihistamine. Taking it also seems to help get past those sleep onset events. I have the same thing but mine is resolved using the machine, naps without the machine is another story.
6. I would see your doctor including your GP about a trial on Provigil, hammer hard for it, you can read up on it below,
http://www.provigil.com/default.aspx
The Sandman Auto will do a couple things for you,
1. Address the obstructive aspect of your disorder from the full range of pressure.
2. Ignore any aspect of Central apnea seen, have the ability to record such activity including mixed events.
3. Allow you to use a lower pressure and help with complications from aerophagia.
4. IF other events are triggers such as FL runs you can fine tune this machine in how you want it to respond, with the
great details it gives in the reports that should be easy. Very easy machine to program.
5. Sandman will be much quieter at its lower pressure than even AFLEX. If the M series was quiet Respironics wouldn't have come out
with a noise silencer, they did that due to complaints of it being noisy. My 420e is quieter than my AFLEX. Higher the pressure the more
noisy they all are.
Last edited by Snoredog on Fri Nov 07, 2008 3:46 pm, edited 1 time in total.
someday science will catch up to what I'm saying...