







Snoredog,
Just to add some proof to fitness, did this jump (see 'Skyjump') twice in 15 mins four weeks ago. What might be referred to as an unusual form of forced ventilation
http://www.skycityauckland.co.nz/skycit ... s_home.cfm
http://www.skyjump.co.nz/
Doug
Why doesn't APAP respond to apneas?
Re: Why doesn't APAP respond to apneas?
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)

Re: Why doesn't APAP respond to apneas?
Thanks for setting me straight. Glad I checked before I went to bed.
Also, I've gained a little weight since I started all of this. I now weigh 139 pounds , about what I weighed when I was last 9 months pregnant 28 years ago. Sigh.....
Bev
OMG, Doug, your wife lets you do that??!!!!
Also, I've gained a little weight since I started all of this. I now weigh 139 pounds , about what I weighed when I was last 9 months pregnant 28 years ago. Sigh.....
Bev
OMG, Doug, your wife lets you do that??!!!!
Diagnosed 9/4/07
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1

Re: Why doesn't APAP respond to apneas?
Hey don't feel bad, I was in the Mall today without my glasses, just looking at everything, walk by this one shop had some mannequins with some nice sweaters on them, looked closer they had a pop belly, I said to myself lookie there, I know there is a obesity epidemic but they are even portraying that on mannequins, then I realized it was a maternity shop good thing I didn't walk in to look at them closerOutaSync wrote:Thanks for setting me straight. Glad I checked before I went to bed.
Also, I've gained a little weight since I started all of this. I now weigh 139 pounds , about what I weighed when I was last 9 months pregnant 28 years ago. Sigh.....
Bev
OMG, Doug, your wife lets you do that??!!!!
someday science will catch up to what I'm saying...
Re: Why doesn't APAP respond to apneas?
OutaSync wrote: <snip>
OMG, Doug, your wife lets you do that??!!!!
NUP, she was in Japan - I was in NZ, I didn't tell her until a few days after we got back together in Australia
But, my 2 sons & one of them's fiancee were there to film it
Reason I did it twice was after landing from 1st go, they asked me if I'd ever do it again - "yes" - then go have another free go - am guessing it was a way to attract more customers as I was the only person lined up to jump that afternoon. If an ole grandad man can do it, anyone can
DSM
PS, I asked them how old the oldest jumper had been (thinking at my age I might be somewhere near being their oldest client) - the surprise was when they claimed a 92 year old had done the jump only a few months before.
Last edited by dsm on Wed Oct 29, 2008 6:26 pm, edited 1 time in total.
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
Re: Why doesn't APAP respond to apneas?
Snoredog, you crack me up!
BTW, I just found out that you can't set EPAP higher than IPAP Min. It won't let you. It changed IPAP Min and Max for me.
Bev
BTW, I just found out that you can't set EPAP higher than IPAP Min. It won't let you. It changed IPAP Min and Max for me.
Bev
Diagnosed 9/4/07
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Re: Why doesn't APAP respond to apneas?
I agree, from Bev's picture it appears she is at ideal weight, so with that in mind for 67" tall person, I show she should be around 530ml, she is well below that. But as SWS suggested she also appears to be a petite person and can easily have lower lung capacity, so the guides could be off.Banned wrote:I know you all think Bev's Tidal Volume is ok, and maybe it is, but save for one occurrence that indicated a VT 420ml, she is generally at the very low end of her 5 kg VT minimums. I guessed her Frame: Medium, Height: 5' 7", Weight 120lbs. The 5kg minimum for someone of this stature is 337ml. The light VT maybe worth watching. http://www.healthcentral.com/diet-exerc ... 6-143.html
Banned
At last SV mode test, the machine also thought she needed her peak volume up and it did a lot of pegging at the IPAP Max, this sent her into periodic breathing and central dysregulation. I suspect it did that by over-targeting her peak volume, so I believe the thought was to increase EPAP and hopefully prevent that over-targeting and settle down IPAP working a bit. She recovered from the Central Dysregulation pretty fast, but machine had a tough time stabilizing her.
First night report as at a much lower pressure at 9 cm and standard protocol settings for the machine, my opinion is she didn't do bad there, not great but also not bad. IPAP was still pretty busy.
someday science will catch up to what I'm saying...

Re: Why doesn't APAP respond to apneas?
Yeah, she would definitely feel 530 ml. My max Average Tidal Volume would be 550 ml and I'm 5'11". dsm has an Average Tidal Volume of 650ml. People's lung capacity are different, as I'm learning.Snoredog wrote: I, show she should be around 530ml, she is well below that. But as SWS suggested she also appears to be a petite person and can easily have lower lung capacity, so the guides could be off.
I think AVAPS would be a better bet for Bev, than the SV. I would trial Bev for two weeks in S/T machine to get a good baseline Average Tidal Volume. Than inflate her to no more than 10% over baseline using AVAPS.
AVAPS couldn't make any worse of a door stop than the SV.
Banned
AVAPS: PC AVAPS, EPAP 15, IPAP Min 19, IPAP Max 25, Vt 520ml, BPM 10, Ti 1.8sec, RT 2 (Garage)
BiPAP Auto SV: EPAP 9, IPAP Min 14, IPAP Max 25, BPM 10, Ti 2sec, RT 2 (Travel Machine)
VPAP Adapt SV: EEP 10.4, Min PS 4.4 (Every Day)
Mask: Quattro
BiPAP Auto SV: EPAP 9, IPAP Min 14, IPAP Max 25, BPM 10, Ti 2sec, RT 2 (Travel Machine)
VPAP Adapt SV: EEP 10.4, Min PS 4.4 (Every Day)
Mask: Quattro
Re: Why doesn't APAP respond to apneas?
I think you are right on the AVAPS, it targets tidal volume as opposed to peak and uses an average to bring it up with pressure support. That seems what Bev needs an avg. based upon tidal and maybe Pressure Support wouldn't be so radical. That rapid moving pressure support seems to be what destabilizes her breathing.Banned wrote:Yeah, she would definitely feel 530 ml. My max Average Tidal Volume would be 550 ml and I'm 5'11". dsm has an Average Tidal Volume of 650ml. People's lung capacity are different, as I'm learning.Snoredog wrote: I, show she should be around 530ml, she is well below that. But as SWS suggested she also appears to be a petite person and can easily have lower lung capacity, so the guides could be off.
I think AVAPS would be a better bet for Bev, than the SV. I would trial Bev for two weeks in S/T machine to get a good baseline Average Tidal Volume. Than inflate her to no more than 10% over baseline using AVAPS.
AVAPS couldn't make any worse of a door stop than the SV.
Banned
The AVAPS manual is an interesting read, they should allow a person to rent one of these machines before purchasing. Rent-A-Pap.
I wonder how Bev would do with lower settings and greater pressure support, we've seen what she does at baseline, 1 cm delta, 2 cm delta 4 cm delta on her PSG's. Wonder what she would do with 14/6 or something similar like the AVAPS shows with 8 cm PS with BPM=10. That would bring her tidal volume up.
I think when people breathe shallow that the machine needs to help keep them breathing deeper with pressure support, adjustment of Inspiration timer and a low exhale pressure.
someday science will catch up to what I'm saying...
-
StillAnotherGuest

- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
"Then Gimme A Freebie"
Use all these points, but hammer the inadequacy of the REM analysis (no REM in split, severely-delayed and inadequate quantity in the BiPAP titration). If he says, "Yeah, we had a little", then say, "Great, but in the BiPAP titration, the pressures utilized were 21/17, 23/19 and 25/21, and the AHI was still 27.7. What's up with that?"OutaSync wrote:Right now, I have to get enough information together to convince my insurance company that I need to have another sleep test. I would have to have a referral, and since my current sleep doctor thinks I'm "fine" and "doing well", I doubt I'll get one from him. But he has partners, who are more experienced, so if I could make my case, with facts and figures from the same sleep studies that the doctor reviewed, maybe I could get somewhere.
Clearly defining the extent of disease in REM will also go a long way in determining the extent (or existence) of CompSAS.
SAG

Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Looking Ahead...
Or simply, the problem is with sleep and not sleep-disordered breathing.-SWS wrote:SAG, you speculated about latent or non-existent arousals in response to OA or CA. I personally suspect that part of the theoretical analysis might very well be correct. Let's assume that it's correct for this particular line of inquiry: At this point of our theoretical analysis we have choreographed: 1) an apnea with 2) a latent or remiss arousal/awakening mechanism, and 3) consequential desaturation.
We still have a couple paradoxes on our hands, though:
1) Excessive RDI- If arousals are not occurring as a timely response to help mitigate apneic desaturations, then why might they be occurring in such large numbers for complex SDB patients? What might the stimuli-related mechanism be in complex SDB pathophysiology to cause an excessive RDI that seems to not resolve A or H---and at the same time will not be satisfactorily mitigated with PAP?
2) Minimal AHI in cases of slight CompSA/CSDB- Is this actually a paradox regarding complex SDB? Or is AHI scoring simply too time-permissive or coarse regarding perhaps extremely short, sudden disruptions to both eupneic breathing and sleep drive?
Again, I believe minimal compSA/CSDB AHI can sometimes be attributed to a non-linear pressure relationship regarding nothing more than minimization of the frank A and H part of CompSA/CSDB pathophysiology---with that pressure-related "saddle-point" not necessarily having successfully mitigated the excessive RDI/RERA component of compSA/CSDB.
I think that may be what's happening in Bev's case as she sits around 14 cmH2O with a great AHI and yet highly deteriorated overall sleep---deteriorated presumably because of an unresolved RDI/RERA component that is both excessive and typical of CompSA/CSDB.
Regardless, this will be a great discussion for the winter "Hot-Stove Sessions" and should turn this into the TMOTMOAT!
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
Re: Why doesn't APAP respond to apneas?
I had a terrible time last night. Couldn't get to sleep. First there was this loud rushing sound. I thought, WOW, 15 has much noisier exhaust than 14. After awhile I couldn't sleep through the noise, so got up and switched cushions. BINGO, it had been a leak in the cushion. Can't see anything wrong with it this morning. It was very hard to breathe against the pressure. This morning I realized that I had my settings wrong, I guess when I was experimenting to see if you could set the exhale higher than the inhale, I thought I had changed everything back to 15, but somehow it was on 16 all night, which Encore reports as 17. Keep in mind that 16 is what my prescription is for. No wonder I couldn't tolerate that on straight CPAP. It was a horible night. Even with my Activa strapped down so tight my teeth hurt, it was still leaking. Don't tell me that the Activa floats on the face and you have to wear it loose. That is SO not true for me. I have tried it every which way, over the last year, and the only way it won't leak for a few hours at a time is to clamp it down tight. The skin on my nose bridge peels, even with the pad a cheeks nose bridge guard.
So here is last night:
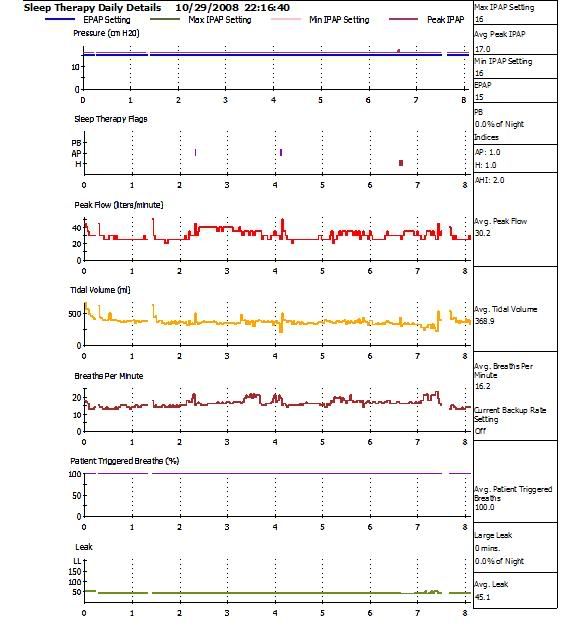
BTW, I'm not going to take that LYrica anymore. It dragged me out so much I almost ran through a red light yesterday on a route that I take every day. Screeched my tires and stopped on the other side of the crosswalk. It didn't even register that the light was red until a car passed in front of me. In the second that I wondered why that car was going when I was going, I realized that my light was red. Good thing it was in the City and I was only going 25 mph,
Bev
So here is last night:
BTW, I'm not going to take that LYrica anymore. It dragged me out so much I almost ran through a red light yesterday on a route that I take every day. Screeched my tires and stopped on the other side of the crosswalk. It didn't even register that the light was red until a car passed in front of me. In the second that I wondered why that car was going when I was going, I realized that my light was red. Good thing it was in the City and I was only going 25 mph,
Bev
Diagnosed 9/4/07
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Re: Why doesn't APAP respond to apneas?
sorry you had a rough night Bev,
I would go back on the Aflex for a day or two and catch back up on your sleep.
You also NEED to use a Ramp, set it at 8 or 9 (or what ever is comfortable) for at least 30 minutes, use of Ramp won't impact your results at all but it will make it easier to fall asleep. Set up and use the ramp with either machine, would rather see you use Ramp than prescription drugs.
If that Lyrica is knocking you out during the day stop taking it. That was the idea behind aspirin and melatonin to see if it would improve your daytime fatigue. A lot of the daytime fatigue can be from the Ambien and/or other medications.
I would go back on the Aflex for a day or two and catch back up on your sleep.
You also NEED to use a Ramp, set it at 8 or 9 (or what ever is comfortable) for at least 30 minutes, use of Ramp won't impact your results at all but it will make it easier to fall asleep. Set up and use the ramp with either machine, would rather see you use Ramp than prescription drugs.
If that Lyrica is knocking you out during the day stop taking it. That was the idea behind aspirin and melatonin to see if it would improve your daytime fatigue. A lot of the daytime fatigue can be from the Ambien and/or other medications.
someday science will catch up to what I'm saying...
Re: Why doesn't APAP respond to apneas?
Or maintenance of both wake and sleep drive, which is the way that N is so often viewed. I also agree that there are multiple reasons to see PSG REM distribution without the skewing effects of Lexapro. If Narcolepsy is involved, psychological stressors alone can exacerbate daytime somnolence.SAG wrote:Or simply, the problem is with sleep and not sleep-disordered breathing.
I honestly think that's excellent advice.Snoredog wrote:I would go back on the Aflex for a day or two and catch back up on your sleep.
Bev, my vote is that you also go back on your previous APAP 14 - 17 for at least a while. You can wean off Lyrica while catching up on rest, and you can also review the excellent criteria SAG put forth in recent pages to justify that next PSG. Regarding the cost of heading up to Harvard's teaching hospital: the order of cost shouldn't be dissimilar to heading out of town for a Mayo Clinic visit, which I think Slinky is doing right now. By the way, the Mayo Clinic sleep department is another world-class choice regarding researchers who are on the leading edge of understanding complex sleep disordered breathing---which you may or may not have.
Anyway, I sure like the idea of catching up on sleep at APAP 14 -17. Your AutoSV will be there waiting for you after you're good and rested. If you are going to run any more home based SV experiments, then I suggest running them only on weekends---and with just tiny changes at a time.
I also agree that Lyrica's side effects sound adverse. Unfortunately that is a well known side effect that my neurologist was most concerned about as well. I got lucky with Lyrica. But I do know that when I start up Lyrical, I must spend a couple/few days sleeping around 15 or 16 hours---and then I'm much better on Lyrica than off it. Go figure.
Last edited by -SWS on Thu Oct 30, 2008 9:36 am, edited 2 times in total.
Re: Why doesn't APAP respond to apneas?
Thanks, guys, I'll do all of the above. There will be no "weaning" of the Lyrica. I just won't take another one. I was only on for two days and I felt terrible both days. I don't have time to adjust to it. I have to drive and work every day and can't afford to be a basket case all weekend, either.
Thanks, SAG, for taking the time to review my data. I know you are a busy guy, so that meant a lot to me.
Bev
Thanks, SAG, for taking the time to review my data. I know you are a busy guy, so that meant a lot to me.
Bev
Diagnosed 9/4/07
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
Sleep Study Titrated to 19 cm H2O
Rotating between Activa and Softgel
11/2/07 RemStar M Series Auto with AFlex 14-17
10/17/08 BiPAP Auto SV 13/13-23, BPM Auto, AHI avg <1
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
Re: Looking Ahead...
TMOTMOAT might be something to sink one's teeth into and chew the fat on, but it's not something to eat -- which might be what people new to the message board are wondering... "Hmmm... oatmeal with sliced tomatos, maybe?"StillAnotherGuest wrote:Regardless, this will be a great discussion for the winter "Hot-Stove Sessions" and should turn this into the TMOTMOAT!
SAG
TMOTMOAT = "The Mother Of The Mother Of All Threads"
TMOAT itself (herself?) was here:
viewtopic.php?t=11458
Jul 22, 2006 subject: Resmed VPAP Adapt SV - for Central Sleep Apnea
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435