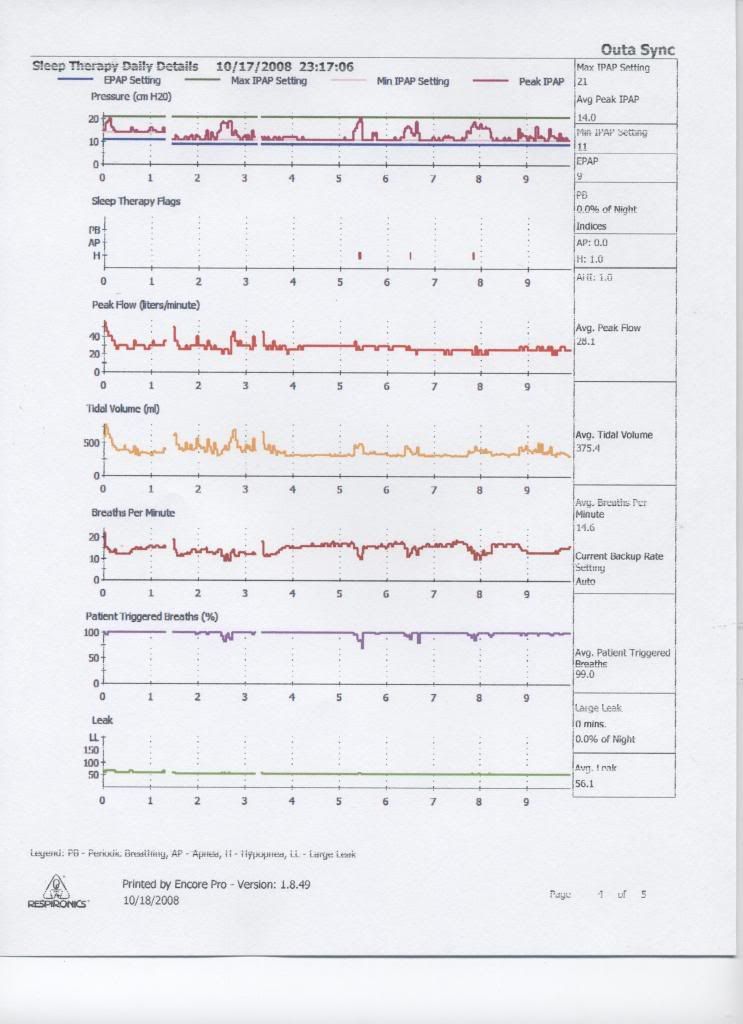
Sorry to hear you had a hard time sleeping, Bev. I'd suggest turning the apnea alarm all the way off (you never had it on your previous machines). Also, it sounds as if IPAP/EPAP pressure cycling kept you awake. That can take some getting used to---especially with IPAP peak fluctuating as much as it did during your attempted sleep session.
It's that fluctuating IPAP peak---let alone while awake--- that can make SV so unfriendly to the wake/stage-1 sleep transition. You may initially need your ambien just to get used to that IPAP peak fluctuation while awake.
On that basis I would suggest initially turning SV completely off while you first learn to sleep with ordinary BiLevel. When it comes to BiLevel, some people may conceivably need to learn how to crawl (with low constant IPAP pressures) before they learn to run (with wildly or dynamically fluctuating IPAP pressures). If you would like to spend a few nights learning how to sleep with basic BiLevel before attempting to try SV modality, then just set IPAP max as low as you have your IPAP min. When IPAP max equals IPAP min, you have SV turned off and you are running at ordinary Bilevel. See if you can learn to sleep with simple BiLevel first, collecting important baseline data along the way.
Then as soon as you get comfortable sleeping with ordinary BiLevel, consider experimentally turning SV modality on, perhaps initially limited to a few cm above IPAP min---then experimentally extend that IPAP max if it feels comfortable.
Toward learning how to fall asleep with ordinary BiLevel: See Dr. Krakow's Pearls of BiLevel therapy posts. Somewhere in this lengthy thread he suggests what patients can do to learn how to comfortably sleep with BiLevel:
viewtopic.php?f=1&t=26896&p=232510#p232510
Also, what's your current rise time? Since you're not primarily a centrally-dyregulated patient, you can experiment with a longer rise time if that's more comfortable. Once you have a comfortable rise time dialed in that doesn't dysregulate, you can use that same rise time when you experimentally turn SV back on. In summary: I suggest that you first get acclimated to just as much as possible (the idea, the smell, the whooshing, the rise time, the slight cycling of ordinary BiLevel, etc.) before finally turning SV on for yet a second acclimation period. That first acclimation period at ordinary BiLevel should also allow you to figure out what fixed BiLevel pressure is just enough to address all your obstructive apneas and hypopneas.
Last but not least, there's always the option of CPAP with SV to eventually try. It's there for a purpose. Some patients find CPAP more comfortable than BiLevel, but still need that SV to occasionally kick in on an as-needed basis.