






Thank you, Bev!OutaSync wrote:Changing my will, now.
Bev
Just kidding, of course! But just in case I wasn't do you have any other cool electronics? I just got a new IPOD, so I'm good there...
Thank you, Bev!OutaSync wrote:Changing my will, now.
Bev
The Navigon 5100!!!!???!! Whoa!!! That's a VERY nice unit! Just a quick rundown of those features:OutaSync wrote:Navigon 5100. Love it. Gives me live traffic info!

Once again, Bev, thank you very much!!! Thank you very much, indeed!!!The Navigon 5100 Sales Brochure wrote: This take anywhere device is simple to use and offers:
* A host of premium features no other GPS offers
* Up to 12 map updates when you accessorize with FreshMaps
* Extra guidance with exclusive 3D Reality View™ and Lane Assist
* Free Lifetime Traffic that works out of the box
* Exclusive Zagat® Ratings and Reviews
* Intuitive menus and stunning 2D and 3D maps
* Easy-to-read map views that adapt to your needs
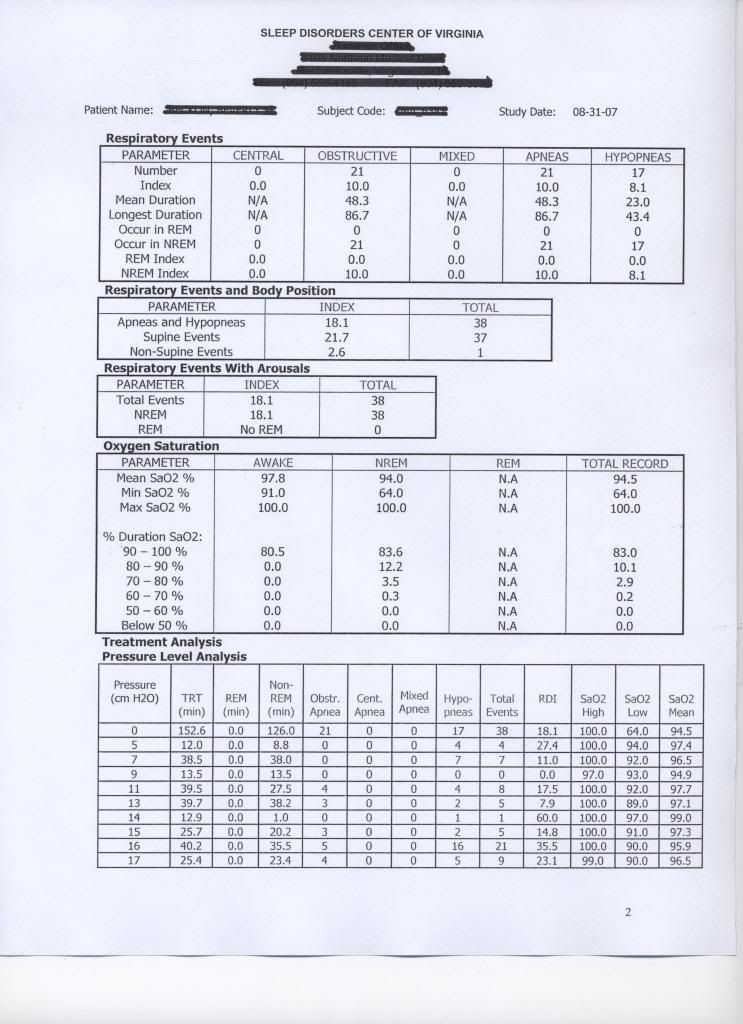
Only problem with that theory is if she blew right past an ideal pressure finding below 14 cm due to centrals seen. You have to consider the machine got to that pressure along the way responding to central apnea with pressure. Granted she did a manual titration with the Minimum pressure observing a false AHI. As you mentioned before if some of those apnea could be neurological based, with increased pressure support and target volume she gets from the SV she may not have had them at all.-SWS wrote:Alright. I just looked at your Encore results on page one of this thread. With pressure endlessly sitting at 14 cm you appear to get a very acceptable AI and HI. There's a slight chance with BiPAP AutoSV that you just may be able to eventually drop below that 14 cm, however.OutaSync wrote:My best pressure range for AHI is what I was using 14-17.
I would like to see us discuss Inspiration Time and how that might change ones breathing to a particular scenario. Respironics keeps resorting to 1.2 seconds when it sees a problem, I wonder why they choose that value? With the range of that setting seems it could vary quite a bit.Settings
– Max IPAP = Min IPAP –30 cmH2O
– Min IPAP = EPAP –30 cmH2O
– EPAP = 4 –25 cmH2O
– Rate = Auto, off, fixed (4 –30 BPM)
– Rise = 1 –6 (100 –600ms)
– Timed Insp = 0.5 –3.0 sec (0.1 increments)
– Ramp Time = 0 –45 min
– Ramp Start = 4 cmH2O –EPAP
– Humidity = off, 1 –5
– Display parameters Pressure, Volume, Leak
I think that's a good idea, Snoredog.Snoredog wrote:I would like to see us discuss Inspiration Time and how that might change ones breathing to a particular scenario.
Well, Respironics is not telling clinicians to set IT at 1.2 seconds, as if that's a magic value. Rather Respironics is saying don't set IT at anything less than 1.2 seconds if the titration-protocol decision branches happen to bring the clinician to that point. The sleep tech will set IT at the appropriate value based on measured respiratory parameters---but no less than 1.2 seconds per Respironics' recommendation.Snoredog wrote:Respironics keeps resorting to 1.2 seconds when it sees a problem, I wonder why they choose that value?
But I do agree that the titration guide can provide help regarding what changes may be necessary when certain things go wrong---such as unresolved PB being scored on the Encore Charts.snoredog wrote:I see nothing wrong with following the lab titration guide, it teaches her on what to change to a particular condition instead of simply guessing.
Doug, I missed that working baseline of 10 for epap. Where is that?dsm wrote:I agree re using Respironics recomm titration - but, I would start Bev off at around 10 for epap as we already have a working baseline.
I also missed the significance of 10 cm in the BiPAP AutoSV patent descriptions and manufacturer literature. What's the significance of EPAP at 10 cm regarding SV design?dsm wrote:I mention 10 also as being a good starting point as knowing how SVs work...
SWS,-SWS wrote:I simply asked Bev what her best results were:
viewtopic.php?f=1&t=35298&start=120#p304114
Bev very simply stated that 14 to 17 yielded her best AHI.
So where does your 10 cm come from? I never got the answer to that one. Just boomerang questions. I wanna know where 10 cm came from in her CPAP titration, and I wanna know how an EPAP of 10 cm relates to the design or operation of SV.


