Well, I continue to look at the Portable Initiatives with great fear and trepidation because the accurate assessment of sleep disorders requires time, effort and knowledge regardless of the actual testing methodology utilized. Clearly, the more abbreviated the test results are, the sharper you have to be in order to accurately interpret them.
If the whole conversation goes like this:
Patient: My wife says I have a problem sleeping.
Physician: Wear this thing tonite and bring it back in the morning.
(Next morning) Physician: Well, your RDI is 10.1. What do you want to do?
the only advantage is that in Portable Testing, you've thrown less money down the toilet.
rooster wrote:Are you speaking of co-morbidities whose primary means of diagnosis are through PSGs? If so, it is very surprising news to me. Please specify what these major co-morbidities are?
Insomnia (if the device doesn't measure actual sleep), medication effect, moderate to severe pulmonary disease, the nocturnal myoclonuses (myocloni?), neuromuscular disease, congestive heart failure and "central dysregulation" (although this is getting tossed around a little too freely. The going estimate of CompSAS hovers around 15%, but what is actually clinically significant is probably much less than that) come to mind.
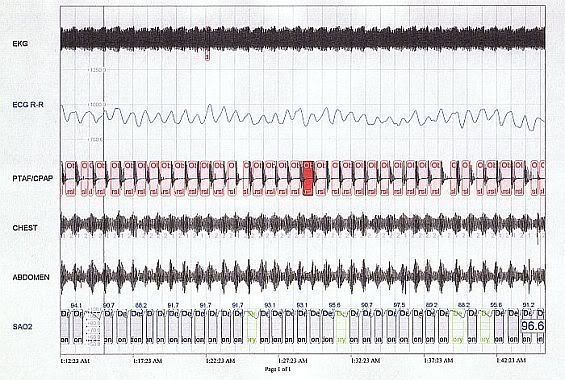
BTW, the whole concept of peripheral arterial tone (PAT) is truly fascinating, and rather than being relegated to portable testing, should be included in "formal testing" (or at least, look at
some measure of autonomic arousal).
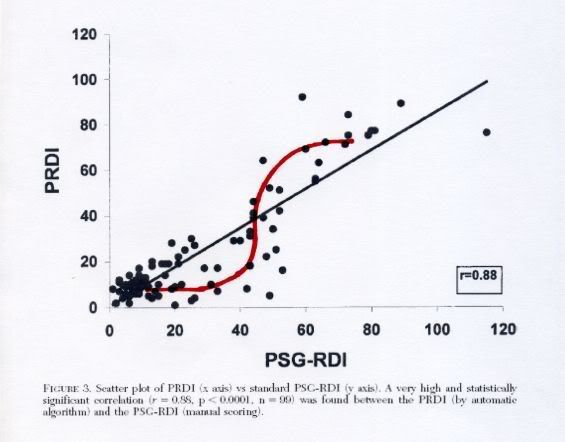
Since the above-noted correlation study, published in
Evaluation of a Portable Device Based on Peripheral Arterial Tone for Unattended Home Sleep Studies,
Amir Bar, MD; Giora Pillar, MD, DSc; Itsik Dvir, DSc; Jacob Sheffy, PhD; Robert P. Schnall, DSc and Peretz Lavie, PhD; Chest. 2003;123:695-703.
I understand that there were improvements in the algorithm, and
Validation a Portable Monitoring Device for Sleep Apnea Diagnosis in a Population Based Cohort Using Synchronized Home Polysomnography Ding Zou, MD; Ludger Grote, MD, PhD; Yüksel Peker, MD, PhD; Ulf Lindblad, MD, PhD; Jan Hedner, MD, PhD; SLEEP, Vol. 29, No. 3, 2006
showed better results in that mild to moderate results range.
SAG