







SWS,
Thanks - good table - very clear. What has caught my eye is this mode
SWS clip "EPAP=7, IPAP min=7, & IPAP max=16: CPAP w/ SV mode (CPAP=7 during non-SV moments, and SV ranging as high as 16/7 on an as-needed basis)"
& I will run my machine tonight set up with Epap=11, IpapMIN=11 & IpapMAX = 20.
The data from such a night is going to be interesting even though I think the mode may prove less comfortable than what am used to.
DSM
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): CPAP
Little Larissa - please read
Last night I set my BipapSV as follows & ran it this way for 3 hours (had to revert due to how uncomfortable it felt despite SV mode being active).
CPAP Mode ... Epap=11, IpapMIN=11 IpapMAX=20
(setting Epap=IpapMin forces Cpap mode. If IpapMAX is also set = Epap then SV mode is deactivated. In this instance I left IpapMAX=20 which keeps SV mode active).
The SV mode PS behaved pretty well much as it usually does. The data shows a more erratic peak flow figure. That stabilized back to normal when I boosted IpapMIN back up to 14 CMs.
This test shows that PS will operate as long as IpapMAX is set higher than IpapMIN. The machine didn't feel good in cpap mode - just not enough pressure - felt like there wasn't enough air, breathing in & out was no big issue, just that missing ipap boost which is very comforting. The leak data was high during the 3 hrs of cpap but stabilized once normal operation was resumed. I put that down to the restlessness induced by changing mode from normal.
The SV feature did its job despite the change to CPAP mode & AI number is so low it is hard to score it (machine data says 1.0 but I can only count 3 events for the night).
http://www.internetage.com/cpapdata/dsm ... 2aug08.pdf
Not sure how this test will help Laryssa but it does show what happens when it is set in CPAP SV mode.
DSM
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): CPAP
CPAP Mode ... Epap=11, IpapMIN=11 IpapMAX=20
(setting Epap=IpapMin forces Cpap mode. If IpapMAX is also set = Epap then SV mode is deactivated. In this instance I left IpapMAX=20 which keeps SV mode active).
The SV mode PS behaved pretty well much as it usually does. The data shows a more erratic peak flow figure. That stabilized back to normal when I boosted IpapMIN back up to 14 CMs.
This test shows that PS will operate as long as IpapMAX is set higher than IpapMIN. The machine didn't feel good in cpap mode - just not enough pressure - felt like there wasn't enough air, breathing in & out was no big issue, just that missing ipap boost which is very comforting. The leak data was high during the 3 hrs of cpap but stabilized once normal operation was resumed. I put that down to the restlessness induced by changing mode from normal.
The SV feature did its job despite the change to CPAP mode & AI number is so low it is hard to score it (machine data says 1.0 but I can only count 3 events for the night).
http://www.internetage.com/cpapdata/dsm ... 2aug08.pdf
Not sure how this test will help Laryssa but it does show what happens when it is set in CPAP SV mode.
DSM
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): CPAP
xPAP and Quattro std mask (plus a pad-a-cheek anti-leak strap)
-
StillAnotherGuest

- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Musings...
Equally, if not more important would be Inspiratory Time, although one cannot exceed an I:E Ratio of 1:1 with that thing. But you'd be looking more for an I:E Ratio of ~1:1.5 or so.Banned wrote:So if 3 would be the average Rise Time for an adult, what would be the average Rise Time for a preschool child?
While this may seem picky, she is (probably) not late, the machine is early. This results in selective hyperventilation. And why the monitor should be pCO2 and not SaO2.-SWS wrote:Essentially, here is what I think is happening with Laryssa's IPAP delivery: 1) she's late for almost every breath, so the machine initiates virtually each breath
The AutoSV already compensates for a 6 foot tubing.Banned wrote:This may be a result of dsm's observation that the BiPAP Auto SV looses 1cmH2O at the mask end of the hose (e.g. no proximal tube). I have no guess where the additional 1cmH2O EPAP (lose) came from.StillAnotherGuest wrote:Now I have a question. Why are we at 16/12 cmH2O IPAP 7 cmH2O EPAP when the original parameters were supposed to be 15/5?
The PSG appears to only have supplemental oxygen as a treatment modality, so other than SaO2, I don't see any parameters on which to base pressure support settings.-SWS wrote:The fact that Laryssa initially achieved her best results during a PSG at 15/5...
Age alone would not change pressure requirements (otherwise, using that formula, Banned would now be at IPAP 56/50 cmH2O EPAP 90 cmH2O). Pressure support is volume-variable, so if lung compliance remains unchanged, increase in age (or size) doesn't automatically require increase in pressure.ozij wrote:Laryssa migrated from 2 year old to 3 year old during that time. Couldn't that be the reason?2) How did the initial PSG recommendation of 15/5 migrate into the currently employed BiLevel values, which happen to function as near-equivalents of ST 16/7 (despite SV modality being turned on simply by setting IPAP min and IPAP max at different values)?
SAG

Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
Re: Musings...
I don't think simple chronology was ozij's intended point. Rather, I think pediatric maturation's potential impact on pathology was the valid point of consideration raised by ozij.StillAnotherGuest wrote:Age alone would not change pressure requirements (otherwise, using that formula, Banned would now be at IPAP 56/50 cmH2O EPAP 90 cmH2O). Pressure support is volume-variable, so if lung compliance remains unchanged, increase in age (or size) doesn't automatically require increase in pressure.ozij wrote:Laryssa migrated from 2 year old to 3 year old during that time. Couldn't that be the reason?2) How did the initial PSG recommendation of 15/5 migrate into the currently employed BiLevel values, which happen to function as near-equivalents of ST 16/7 (despite SV modality being turned on simply by setting IPAP min and IPAP max at different values)?
Simple chronology also leaves us stumped to account for Laryssa's recent change of height----if we similarly attempt to apply Banned's recent rate of change as a benchmark comparison.
But I also appreciate your valid point that pressure changes are not automatically guaranteed to occur with pediatric aging or physical maturation. However, I would think pediatric growth and maturation should gradually influence required pressures more often than not. Laryssa's pathology may or may not be stable, but her pulmonary-related biophysics are not at all static thanks to biologic growth and maturation.
We clearly aren't seeing the majority of medical records (rightly so, considering the nature of this venue). And those PSG excerpts on page one are incomplete. But I would also be a bit curious about the details regarding how/why that initial 15/5 setting was determined.SAG wrote:The PSG appears to only have supplemental oxygen as a treatment modality, so other than SaO2, I don't see any parameters on which to base pressure support settings.

Re: Musings...
Due to my increasing age I have had to raise my EEP to 56 cmH2O and IPAP to 90 cmH2O. I'm thinking I could also use some Average Volume Assured Pressure Support to cope with times I'm not be getting enough air. Would AVAPS help me?StillAnotherGuest wrote: Age alone would not change pressure requirements (otherwise, using that formula, Banned would now be at IPAP 56/50 cmH2O EPAP 90 cmH2O).
SAG
Worst case is I could always give it to Laryssa when she can handle a 200ML volume.
Banned
AVAPS: PC AVAPS, EPAP 15, IPAP Min 19, IPAP Max 25, Vt 520ml, BPM 10, Ti 1.8sec, RT 2 (Garage)
BiPAP Auto SV: EPAP 9, IPAP Min 14, IPAP Max 25, BPM 10, Ti 2sec, RT 2 (Travel Machine)
VPAP Adapt SV: EEP 10.4, Min PS 4.4 (Every Day)
Mask: Quattro
BiPAP Auto SV: EPAP 9, IPAP Min 14, IPAP Max 25, BPM 10, Ti 2sec, RT 2 (Travel Machine)
VPAP Adapt SV: EEP 10.4, Min PS 4.4 (Every Day)
Mask: Quattro
Re: Musings...
Banned wrote:Due to my increasing age I have had to raise my EEP to 56 cmH2O and IPAP to 90 cmH2O.StillAnotherGuest wrote: Age alone would not change pressure requirements (otherwise, using that formula, Banned would now be at IPAP 56/50 cmH2O EPAP 90 cmH2O).
SAG
At ordinary pressures we had to worry about inducing central apneas or even aerophagia. But at 90 cm we may also have to worry about inducing vertical loft.
Houston, I think we have a problem.... Woah!!
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
What's a Draft?
Having been out in the sun all day without a hat, my brain must have gotten a little baked. Can you explain this a little differently? Is Laryssa taller? Is Banned taller? Is Laryssa taller than Banned? Is Banned a "Little Person"?-SWS wrote:Simple chronology also leaves us stumped to account for Laryssa's recent change of height----if we similarly attempt to apply Banned's recent rate of change as a benchmark comparison.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
Sorry about that, SAG. In a nutshell: Any adult, including Banned, cannot be used to demonstrate the effects of pediatric growth on pulmonary-related biophysics.StillAnotherGuest wrote:Can you explain this a little differently?-SWS wrote:Simple chronology also leaves us stumped to account for Laryssa's recent change of height----if we similarly attempt to apply Banned's recent rate of change as a benchmark comparison.
It's a given that pathology and interrelated lung compliance drive pressure requirements. However, pediatric growth alone can have some influencing effect on therapeutic pressures as ozij well pointed out in my opinion. Einstein was famous for running hypothetical "mind experiments" in physics. I think we can also run a hypothetical mind experiment in epidemiology to get a better feel for ozij's intended point:
Take a statistically robust sample of healthy middle-aged adults with perfect lung compliance and absolutely no pulmonary-related pathology. How many of those adults can adaptively sustain expiratory effort during sleep against 10 cmH2O pressure? Now take a statistically robust sample of healthy two-year old children, also with perfect lung compliance and absolutely no pulmonary-related pathology. How many of those two-year old children can adaptively sustain expiratory effort during sleep against 10 cmH2O pressure?
We can't arrive at the exact numbers with the above hypothetical experiment. However, I think we intuitively know that the discrepancy between those two age groups will be vast. I realize that we can nitpick about disruptively applying 10 cmH2O to perfectly healthy subjects---especially pediatric subjects. But in that hypothetical experiment we have removed the interrelated issues of pathology and inadequate lung compliance to reveal that pediatric growth and system maturation alone can have an influencing effect on efficacious pressures.
Conversely, I don't think we can conclude that pathology and lung compliance alone will determine therapeutic pressure changes throughout a pediatric growth curve.
Last edited by -SWS on Sat Aug 16, 2008 7:10 am, edited 1 time in total.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Where AM I?
OK, while I was out in the sun without a hat someone dropped a claw hammer on my head so clearly whatever powers of understanding I had yesterday were... were... what day is today anyway?-SWS wrote:It's a given that pathology and interrelated lung compliance drive pressure requirements. However, pediatric growth alone can have some influencing effect on therapeutic pressures as ozij well pointed out in my opinion. Einstein was famous for running hypothetical "mind experiments" in astrophysics. I think we can also run a hypothetical mind experiment in epidemiology to get a better feel for ozij's intended point:
Take a statistically robust sample of healthy middle-aged adults with perfect lung compliance and absolutely no pulmonary-related pathology. How many of those adults can adaptively sustain expiratory effort during sleep against 10 cmH2O pressure? Now take a statistically robust sample of healthy two-year old children, also with perfect lung compliance and absolutely no pulmonary-related pathology. How many of those two-year old children can adaptively sustain expiratory effort during sleep against 10 cmH2O pressure?
We can't arrive at the exact numbers with the above hypothetical experiment. However, I think we intuitively know that the discrepancy between those two age groups will be vast. I realize that we can nitpick about disruptively applying 10 cmH2O to perfectly healthy subjects---especially pediatric subjects. But in that hypothetical experiment we have removed the interrelated issues of pathology and inadequate lung compliance to reveal that pediatric growth and system maturation alone can have an influencing effect on efficacious pressures.
Conversely, I don't think we can conclude that pathology and lung compliance alone will determine therapeutic pressure changes throughout a pediatric growth curve.
O. said:
To whichozij wrote:Laryssa migrated from 2 year old to 3 year old during that time. Couldn't that be the reason?2) How did the initial PSG recommendation of 15/5 migrate into the currently employed BiLevel values, which happen to function as near-equivalents of ST 16/7 (despite SV modality being turned on simply by setting IPAP min and IPAP max at different values)?
Now, my understanding of compliance in children is that it actually increases as the child gets taller:SAG wrote:Age alone would not change pressure requirements (otherwise, using that formula, Banned would now be at IPAP 56/50 cmH2O EPAP 90 cmH2O). Pressure support is volume-variable, so if lung compliance remains unchanged, increase in age (or size) doesn't automatically require increase in pressure.
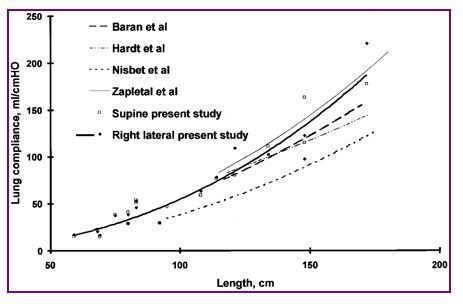
but Laryssa would have needed to get quite a bit taller from her 87 cm in the last 14 months (hence my question, "Did Laryssa get taller?") before this would start to become significant. However, increased compliance would suggest the need for less PS, and not more.
Anyway, present PS might be optimal, so the parameter that would need to be adjusted would probably have to be rate instead of pressure during the "maturation" process.
If the goal of her therapy is pCO2 control, then alveolar ventilation must be consistently maintained. Since pressure-controllled ventilation is volume-variable, there may be huge variations in volume. If we are to take take the volumes from the Encore Reports, we can see tidal volume and minute ventilation all over the place (although the margin of error for these measurements has got to be enormous). This underscores the need for guaranteed volume and pCO2 monitoring, and avoiding any suggestion of "Well, it's been 14 months, so let's add a couple of cm".
Finally, a good way to mess up compliance is to arbitrarily toss in unnecessary EPAP.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
Re: Where AM I?
I think what happened is that adorable baby!StillAnotherGuest wrote:OK, while I was out in the sun without a hat someone dropped a claw hammer on my head so clearly whatever powers of understanding I had yesterday were... were... what day is today anyway?
Although I can only understand about every 20th word you folks are exchanging on this thread, I'm enjoying following it and especially think it's great how the group of you are thinking through and helping to guide Laryssa's therapy.
Mindy
_________________
| Mask: Swift™ FX Bella Nasal Pillow CPAP Mask with Headgears |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Pressure 7-11. Padacheek |
"Life isn't about waiting for the storm to pass, it's about learning how to dance in the rain."
--- Author unknown
--- Author unknown
Re: Little Larissa - please read
SAG, yet another extremely helpful post... Thanks once again!
-
Guest
Re: Where AM I?
Wow.. there are huge variations in Laryssa's average tidal volume (including everything else). But, an ST (Synchrony) machine will never guarantee consistent tidal volume for her, and that maybe what she needs?StillAnotherGuest wrote: If the goal of her therapy is pCO2 control, then alveolar ventilation must be consistently maintained. Since pressure-controllled ventilation is volume-variable, there may be huge variations in volume. If we are to take take the volumes from the Encore Reports, we can see tidal volume and minute ventilation all over the place (although the margin of error for these measurements has got to be enormous). This underscores the need for guaranteed volume and pCO2 monitoring, and avoiding any suggestion of "Well, it's been 14 months, so let's add a couple of cm".
Finally, a good way to mess up compliance is to arbitrarily toss in unnecessary EPAP.
SAG
My understanding is that target tidal volume is 8 ml per kg of ideal body weight (height-weight).
With that in mind, my own average tidal volume is consistently 150 ml below my target tidal volume of 650 ml. Restrictive maybe?
Hence, the SV has been fun with <1 AHI and no gasping issues for me, but maybe AVAPS would offer a better volume solution.
Thanks SAG.
Banned
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
On Various &c
Keep in mind Degree of Accuracy (or "Margin of Error", depending on how you look at it), which, at those Flows and Volumes, is significant:Banned - Guested wrote:there are huge variations in Laryssa's average tidal volume (including everything else).
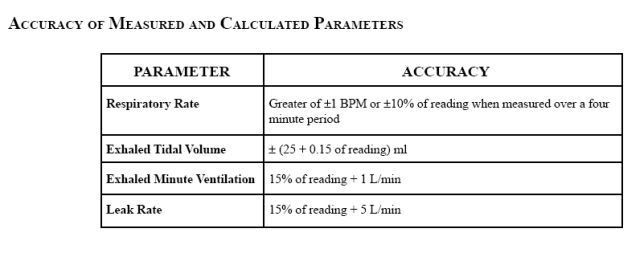
assuming that these values even apply at very low volumes. Reporting out in multiples of 5 LPM, forget the whole Peak Flow thing.
Synchrony is also fixed-pressure/volume-variable with the same Degree of Accuracy, so the same variability will be there. The advantage of Synchrony is that it doesn't have an SV button.Banned - Guested wrote:But, an ST (Synchrony) machine will never guarantee consistent tidal volume for her, and that maybe what she needs?
But yes, in this case, fixed-volume/pressure variable should be a better approach. There is an ETCO2 monitor down there, dig it out and monitor for a few nights. (More assumptions-- assuming that the underlying issue involves chronic respiratory failure)
That's the AVAPS Target recommendation. A completely spontaneous breath would be more in the neighborhood of 5 ml/kg.Banned - Guested wrote:My understanding is that target tidal volume is 8 ml per kg of ideal body weight (height-weight).
Due to high demand for internet interpretation of Pulmonary Function Values, I'm forced to charge a small fee...Banned - Guested wrote:With that in mind, my own average tidal volume is consistently 150 ml below my target tidal volume of 650 ml. Restrictive maybe?
You only need a volume solution if you have a volume problem.Banned - Guested wrote:maybe AVAPS would offer a better volume solution.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
Re: On Various &c
Hmmm. Something about that sounds vaguely familiar...StillAnotherGuest wrote:You only need a volume solution if you have a volume problem.
SAG
Something like, "Gotta know what needs treating, before...." etc.
StillAnotherGuest wrote:Due to high demand for internet interpretation of Pulmonary Function Values, I'm forced to charge a small fee...
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Re: On Various &c
I'll be trailing a Respironics AVAPS machine tonite.rested gal wrote:Hmmm. Something about that sounds vaguely familiar...StillAnotherGuest wrote:You only need a volume solution if you have a volume problem.
SAG
Based on what I have learned here, I'll run my initial (self) titration tonight at:
Mode: S/T AVAPS
EPAP: 11 cmH2O
IPAP Min: 17 cmH2O
IPAP Max: 25 cmH2O
Tidal Volume (Vt): 630 ml
Breath Rate (BPM): 15
Inspiratory Time (Ti): 1.8 (seconds)
Rise Time: 6 (0.6 second)
The AVAPS appears to be an all manual set-up. No AUTO BPM. Not exactly a set-it and forget it machine. Allot more dial winging than the simple ResMED VPAP Adapt SV, so it should be right up my alley. My plan is to dial it in for comfort and check the numbers (as usual).
The only downside to this particular copy of the AVAPS is when you turn the machine 'on' the motor slams against the inner housing. As long as it isn't going through the housing, it should be good to go. There is also no way to get the machine out of 'Provider' mode no matter when or how long you press the 'Silence' button. Hey, it's a Respironics machine, but on the bright side, I can crank up the Tidal Volume and wear a Mirage Micro nasal mask with no alarms.
Banned
Last edited by Banned on Mon Sep 01, 2008 6:18 pm, edited 1 time in total.
AVAPS: PC AVAPS, EPAP 15, IPAP Min 19, IPAP Max 25, Vt 520ml, BPM 10, Ti 1.8sec, RT 2 (Garage)
BiPAP Auto SV: EPAP 9, IPAP Min 14, IPAP Max 25, BPM 10, Ti 2sec, RT 2 (Travel Machine)
VPAP Adapt SV: EEP 10.4, Min PS 4.4 (Every Day)
Mask: Quattro
BiPAP Auto SV: EPAP 9, IPAP Min 14, IPAP Max 25, BPM 10, Ti 2sec, RT 2 (Travel Machine)
VPAP Adapt SV: EEP 10.4, Min PS 4.4 (Every Day)
Mask: Quattro