







So I think, Snoredog, that you are recommending I lower the maximum pressure to 11. And since I was having more events before when I had the lower pressures with the doc starting me at 6 (where I can hardly breathe, BTW), would a range of 8-11 be good do you think? Or could I even do a 9-11 or 10-11? I'd appreciate your input!
Peggy
Wigged out about central apneas
Bravo, Peggy.
Here's a synopsis of a longer post I wrote about setting up the PB420E in auto mode.
I've been a user of the PB 420E auto for 3 years, and had been doing some reading about it. I'm not a sleep professional in any way. My recent reading has convinced me the PB algorithm was planned for a special kind of setup.
When setting up the PB 420E (Puritan Bennett with the Evolution Algorithm) there are 4 different pressures you should look at:
Initial - where the machine goes when you turn it on and when the ramp is finished
Ramp - can start as low as you want, and you can make it lower than the minimum
Minimum - the lowest pressure the machine will go down to when in therapy mode
Maximum - the highest pressure the machine will go up to when in therapy mode
4 different pressures to set.
When PB submitted the machine to the FDA, the automatic mode's function was described as follows:
(my emphasis added:)
http://www.fda.gov/cdrh/pdf3/k031470.pdf
When you don't set an initial pressure, initial and min. default to same. Meaning that you are set up for a slow rise (inhibiting the machine's preemptive capabilities) and speedy decrease back to your minimum - with not much chance of stabilizing around a preferred pressure, since the machine assumes preferred=min.
If you do set up an initial pressure, and make sure it is higher than the minimum, an closer to your preferred or prescribed pressure therapy will start at that pressure, and the pressure will drop if there are indications of airway stability. Once below the initial pressure, the machine will be more responsive to flow limitations, snores etc. On reaching the initial pressure, the rate of change upwards will slow down, and further pressure will be added more carefully, Once higher than your preferred pressure, it will drop back to that quickly and then drop further more carefully.
The bottom line is that you have more chances of staying at or below an optimal pressure if you tell the machine what that optimal pressure is - and you do that by setting it as the initial pressure.
The difference in rate of change is true for all breathing events. Not setting up the initial pressure therefore hobbles the PB's ability to respond quickly to apnea precursors. And also hobbles its ability to respond differently when below the optimum and when above it
Now, the machine does start therapy mode out at initial pressure. Which is why ramp is crucial (not optional) in this automatic machine. If your initial pressure is too high for comfort, you use the ramp to fall asleep. The machine checks your breathing at optimal pressure, and will gladly drop you down if everything is OK.
In summary:
Initial - where the machine goes when you turn it on and when the ramp is finished - (I now set it up with the pressure recommended in my PSG)
Ramp - can be handled like any ramp - based on comfort.
Minimum - the lowest pressure the machine will go down to when in therapy mode - you may want this for many comfort reasons.
Maximum - the highest pressure the machine will go up to when in therapy mode - you may want this for those times your initial is not enough.
I would start out buy letting the PB suggest a 90% pressure - put your PSG pressure in initial, 1-2 less in minimum, and 1-2 more in minmum. The next step will be dealing with the maximum pressure for command on apnea -
Share your data with us so we can figure out how to go from there....
Gee... some auto's on this forum really have a way of going on trips... Like rested gal's Respironics auto... that PB must be learning from it.
O.
Here's a synopsis of a longer post I wrote about setting up the PB420E in auto mode.
I've been a user of the PB 420E auto for 3 years, and had been doing some reading about it. I'm not a sleep professional in any way. My recent reading has convinced me the PB algorithm was planned for a special kind of setup.
When setting up the PB 420E (Puritan Bennett with the Evolution Algorithm) there are 4 different pressures you should look at:
Initial - where the machine goes when you turn it on and when the ramp is finished
Ramp - can start as low as you want, and you can make it lower than the minimum
Minimum - the lowest pressure the machine will go down to when in therapy mode
Maximum - the highest pressure the machine will go up to when in therapy mode
4 different pressures to set.
When PB submitted the machine to the FDA, the automatic mode's function was described as follows:
(my emphasis added:)
http://www.fda.gov/cdrh/pdf3/k031470.pdf
The above mentioned prescribed reference pressure is the 420E's initial pressure.The GoodKnight 420 Evolution can operate in either Constant or Automatic mode. In Constant mode, the device delivers a constant positive airway pressure to the patient at a fixed level prescribed by the practitioner between 4 and 20 cmHrO. In Automatic mode (APAP mode), the practitioner sets a maximum and minimum pressure range above and below the prescribed reference pressure and between 4 and 20 cmHz0. The pressure is adjusted within this range according to the patient’s respiratory pattern and the type of respiratory events detected. Data concerning the type of events detected, their frequency and duration, etc. is stored in the device data memory and can be accessed by the practitioner through the use of the optional Silverlining'" software. Pressure delivery for the GoodKnight 420 Evolution is regulated by a pressure sensor which monitors both ambient and output pressure and provides feedback to the control system.
When you don't set an initial pressure, initial and min. default to same. Meaning that you are set up for a slow rise (inhibiting the machine's preemptive capabilities) and speedy decrease back to your minimum - with not much chance of stabilizing around a preferred pressure, since the machine assumes preferred=min.
If you do set up an initial pressure, and make sure it is higher than the minimum, an closer to your preferred or prescribed pressure therapy will start at that pressure, and the pressure will drop if there are indications of airway stability. Once below the initial pressure, the machine will be more responsive to flow limitations, snores etc. On reaching the initial pressure, the rate of change upwards will slow down, and further pressure will be added more carefully, Once higher than your preferred pressure, it will drop back to that quickly and then drop further more carefully.
The bottom line is that you have more chances of staying at or below an optimal pressure if you tell the machine what that optimal pressure is - and you do that by setting it as the initial pressure.
The difference in rate of change is true for all breathing events. Not setting up the initial pressure therefore hobbles the PB's ability to respond quickly to apnea precursors. And also hobbles its ability to respond differently when below the optimum and when above it
Now, the machine does start therapy mode out at initial pressure. Which is why ramp is crucial (not optional) in this automatic machine. If your initial pressure is too high for comfort, you use the ramp to fall asleep. The machine checks your breathing at optimal pressure, and will gladly drop you down if everything is OK.
In summary:
Initial - where the machine goes when you turn it on and when the ramp is finished - (I now set it up with the pressure recommended in my PSG)
Ramp - can be handled like any ramp - based on comfort.
Minimum - the lowest pressure the machine will go down to when in therapy mode - you may want this for many comfort reasons.
Maximum - the highest pressure the machine will go up to when in therapy mode - you may want this for those times your initial is not enough.
I would start out buy letting the PB suggest a 90% pressure - put your PSG pressure in initial, 1-2 less in minimum, and 1-2 more in minmum. The next step will be dealing with the maximum pressure for command on apnea -
Share your data with us so we can figure out how to go from there....
Gee... some auto's on this forum really have a way of going on trips... Like rested gal's Respironics auto... that PB must be learning from it.
O.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Not only a gentle woman (in reference to my PDF thread gaffe, of course )but a very smart woman, O.! I didn't know if it was okay to say.
Thank you for the explanations about the PB 420E! Wow, it's way more complicated then my M Series! I will probably run the settings by you all before I crank it up for the first time, just to be safe, because even with that wonderful explanation, I'm still not confident I won't screw it up. Lately my brain is kind of mushy. Go figure!
Peggy
Thank you for the explanations about the PB 420E! Wow, it's way more complicated then my M Series! I will probably run the settings by you all before I crank it up for the first time, just to be safe, because even with that wonderful explanation, I'm still not confident I won't screw it up. Lately my brain is kind of mushy. Go figure!
Peggy

it takes a while to find your central threshold, you just want to avoid those pressures that cause the unstable sleep, yours from that report is 13 cm. If you are wondering WHY the machine went up to 13 cm you only have to observe the VS or snores, machine was probably chasing a snore that sent things over the edge. You'll notice between the quiet period between therapy hour 3 and 5.5 there isn't a lot of snoring going on so things are relatively quiet. What pressure were you at there? Probably close to the Minimum pressure is my guess, so I would leave any Minimum pressure where you have it.pjwalman wrote:So I think, Snoredog, that you are recommending I lower the maximum pressure to 11. And since I was having more events before when I had the lower pressures with the doc starting me at 6 (where I can hardly breathe, BTW), would a range of 8-11 be good do you think? Or could I even do a 9-11 or 10-11? I'd appreciate your input!
Peggy
Once you get above 10 cm pressure, the risk of those centrals showing up greatly increases, that is why xpap mfgs. use it in their algorithms so much. Many like the Resmed Vantage refuse to respond to apnea above 10 cm. ...there is a reason for it.
this doesn't mean you have some neurological problem, some people can go up to 20 cm and higher and never see one, but in your case get above 10 and you have a greater risk of them showing up. I see them as a sign of unstable sleep, so to get better sleep you avoid the conditions that lead to or create unstable sleep, in your case keeping pressure below 13 cm would seem to help.
So what you have a couple "true" obstructive apnea left untreated at above 10 cm pressure, that is still better than your brain disliking the current situation so much that it resorts to stopping you from breathing. Central Apnea is perfectly natural, it is the way your brain controls CO2 levels when things aren't going exactly the way it wants.
Even at 8 cm or 10 pressure you will still be getting much more oxygen than without the machine, so you have already removed the most critical adverse factor.
But at the same time the machine is a robot, it sees specific conditions it wants to respond to like FL, like snore. The brain is different, it says hey I'm getting too damn much CO2 flushed out of my blood stream from that machine, so to increase that back up i'm going stop breathing for awhile that will let it build back up, once level returns it starts you breathing again. That brain is pretty smart, if it doesn't see the proper blood flow with the right amount of oxygen it may increase or decrease the rate your heart beats, that will speed up or slow down the amount of blood it receives.
Like I said the brain is pretty smart, does no good to fight the brain, you have to fake it out to make it think a condition has been met. For example, if you used a mask interface that retained more CO2, you would probably see those NR's never return on your reports using the same machine.
If you look at the results of that CSDB study, there was a "mad rush" by CPAP mfgs's afterward to redesign their mask exhaust ports, Respironics changed all of theirs, Resmed did the same. If you have a mask with those little tiny square holes as exhaust ports you have one. Some of those other mfgs like the makers of the hybrid don't have a clue. The mask doesn't have to use a series or cluster of tiny square holes to do the job, it just has to better pay attention to exhaust and CO2 washout characteristics.
If I had to guess, I'd say you are using a mask with a high flow rate, that means it flushes out more CO2 vs one that doesn't. A swift is one example, but they have improved even that one since its introduction with a lower flow rate. You can tell the difference with these masks if you switch during the night, the one with the higher flow rate will feel more refreshing and the other stuffy. While that refreshed feeling may feel better your body may rebel with more centrals showing up, you only see that happen with reports. Just think of those poor suckers giving you advise using a Plus machine and no reports they don't have a clue
When you get a 420e with Silverlining you will be able to see that all more clearly.
Right out of the box the 420e is going to do a better job for you, I can tell that just from reading your reports. Oh and I've owned a dozen or more Remstars and EncorePro going back to 1.24.
someday science will catch up to what I'm saying...
Thank you, SnoreDog! I will try making some adjustments until the 420E gets here.
I guess I don't know what I should be going for exactly. I've been thinking that it's a low AHI like I see some of the lucky folks here reporting. But do the centrals wear me out more, wake me up more? Am I fearing them more than I need to? I guess I have this awful feeling that I will not breathe so long that bad things will happen, but that's probably unrealistic. It's just the thought that freaks me out. A couple weeks ago, my husband touched me on the shoulder to wake me. I knew I hadn't been having a nightmare, when he might otherwise wake me up, so I assumed I'd slept through my alarm and started to jump out of bed. He said, "No, no, no. It's not time to go to work. I woke up to that machine just whining and whining. I thought it must be broken until I saw that you were just laying there, not breathing. So I woke you up to breathe." See, that scares me. What if he doesn't hear the machine whine next time?
I just know I don't feel better now after a month of CPAP and I want to get there. I almost feel more tired than I used to, which totally doesn't make sense. I'm not going to quit, though. I've gotten addicted to that air! But I'd sure like to find the magic combination, and I greatly, hugely appreciate all of you and your generosity of spirit to be helping me through!!!
Peggy
Oh, yeah. My mask is now the ZZZ. I love it! It feels pretty much like the other ones I've tried, inside the mask, I mean, except for the Hybrid. I have a helluva time with that one, feeling like I'm suffocating, and I've never made it even two hours with that sucker.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): 420E, CPAP, AHI
I guess I don't know what I should be going for exactly. I've been thinking that it's a low AHI like I see some of the lucky folks here reporting. But do the centrals wear me out more, wake me up more? Am I fearing them more than I need to? I guess I have this awful feeling that I will not breathe so long that bad things will happen, but that's probably unrealistic. It's just the thought that freaks me out. A couple weeks ago, my husband touched me on the shoulder to wake me. I knew I hadn't been having a nightmare, when he might otherwise wake me up, so I assumed I'd slept through my alarm and started to jump out of bed. He said, "No, no, no. It's not time to go to work. I woke up to that machine just whining and whining. I thought it must be broken until I saw that you were just laying there, not breathing. So I woke you up to breathe." See, that scares me. What if he doesn't hear the machine whine next time?
I just know I don't feel better now after a month of CPAP and I want to get there. I almost feel more tired than I used to, which totally doesn't make sense. I'm not going to quit, though. I've gotten addicted to that air! But I'd sure like to find the magic combination, and I greatly, hugely appreciate all of you and your generosity of spirit to be helping me through!!!
Peggy
Oh, yeah. My mask is now the ZZZ. I love it! It feels pretty much like the other ones I've tried, inside the mask, I mean, except for the Hybrid. I have a helluva time with that one, feeling like I'm suffocating, and I've never made it even two hours with that sucker.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): 420E, CPAP, AHI
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
ozij wrote:Gee... some auto's on this forum really have a way of going on trips... Like rested gal's Respironics auto... that PB must be learning from it.
O.
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
first thing to do is not to worry so much about them, they are not going to hurt you based upon the quantity you are showing. I'd forget trying to get down to a zero AHI, those able to reach that can never maintain it for any length of time, they also don't have shallow breathing or a few centrals to contend with.pjwalman wrote:Thank you, SnoreDog! I will try making some adjustments until the 420E gets here.
I guess I don't know what I should be going for exactly. I've been thinking that it's a low AHI like I see some of the lucky folks here reporting. But do the centrals wear me out more, wake me up more? Am I fearing them more than I need to? I guess I have this awful feeling that I will not breathe so long that bad things will happen, but that's probably unrealistic. It's just the thought that freaks me out. A couple weeks ago, my husband touched me on the shoulder to wake me. I knew I hadn't been having a nightmare, when he might otherwise wake me up, so I assumed I'd slept through my alarm and started to jump out of bed. He said, "No, no, no. It's not time to go to work. I woke up to that machine just whining and whining. I thought it must be broken until I saw that you were just laying there, not breathing. So I woke you up to breathe." See, that scares me. What if he doesn't hear the machine whine next time?
I just know I don't feel better now after a month of CPAP and I want to get there. I almost feel more tired than I used to, which totally doesn't make sense. I'm not going to quit, though. I've gotten addicted to that air! But I'd sure like to find the magic combination, and I greatly, hugely appreciate all of you and your generosity of spirit to be helping me through!!!
Peggy
Oh, yeah. My mask is now the ZZZ. I love it! It feels pretty much like the other ones I've tried, inside the mask, I mean, except for the Hybrid. I have a helluva time with that one, feeling like I'm suffocating, and I've never made it even two hours with that sucker.
You may have already been there but your SDB prevents it with those CA events. Your AHI=2.8 can be shallow breathing or centrals of which the machine will never resolve.
you probably won't feel rested with them present, after you get your 420 you will have a better idea of what is happening, you may just be a shallow breather, those would show up to the machine similarly to centrals but the 420 should clearly identify for you.
but again the 420 is going to do a better job at responding to true obstructive events and avoiding response to centrals over current machine, that should result in better sleep.
If it doesn't, at least you will have the reports and ammo you need to go back to your doctor and ask pertinent questions about what is happening.
When you get your 420, I would set it up with a lower Initial pressure of 8.0, set the Max to 15 until you know what it does for a night. You most likely will have to disable IFL1, but try it first enabled. Starting with a lower pressure than currently being used will make up for the exhale relief offered by current machine so you can still fall asleep. We also want to see how you respond with the command on apnea threshold on the machine, it defaults to 10 cm which should be okay at default but starting your initial pressure below that 10 cm value insures the machine will use it if needed.
Don't worry that little machine is easy to set up and pretty forgiving.
someday science will catch up to what I'm saying...

rofl ! Howdy neighbor!rested gal wrote:ozij wrote:Gee... some auto's on this forum really have a way of going on trips... Like rested gal's Respironics auto... that PB must be learning from it.
O.
_________________
| Mask: Mirage Activa™ LT Nasal CPAP Mask with Headgear |
| Additional Comments: HC100 HH, , Activa Orig. (w/Activa LT cushion), Activa LT, Pur Sleep, Pad A Cheeks, |
Joyce
Started using cpap Sept. 12, 2007
Respironics PR System One Bi-Pap Auto w/Flex,pressure of 9/15, do not use ramp
Started using cpap Sept. 12, 2007
Respironics PR System One Bi-Pap Auto w/Flex,pressure of 9/15, do not use ramp
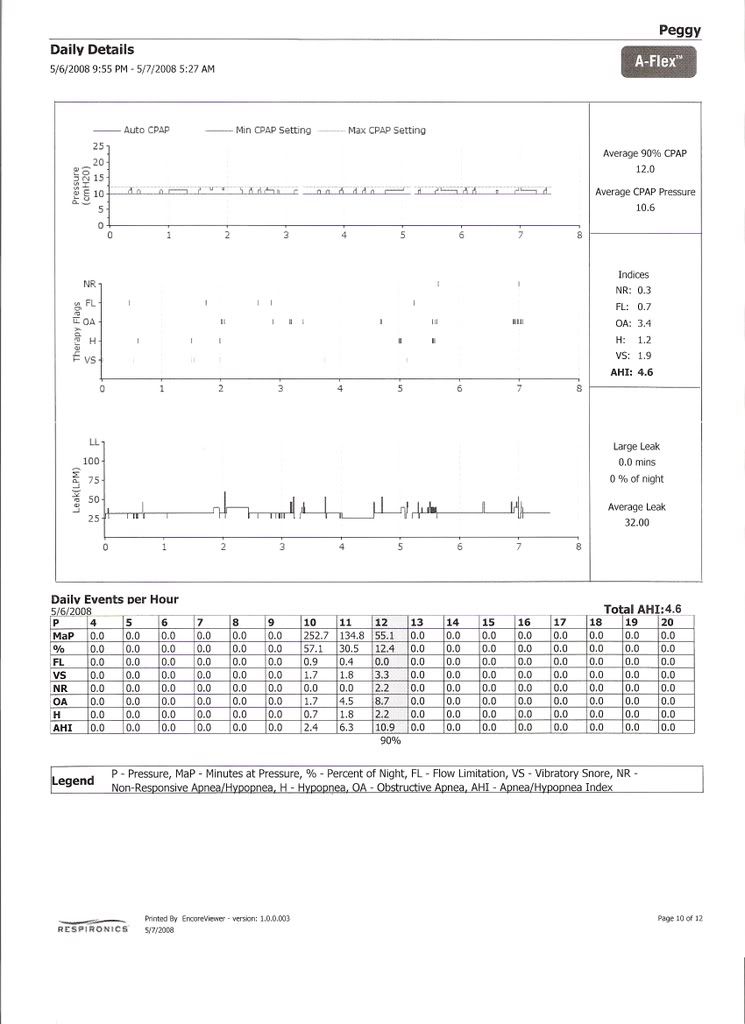
Snoredog, I can see what you're saying about the centrals coming in at the higher pressures and the AHIs being higher there, too, as illustrated by this summary of the last week's use of APAP. But here's the problem. Last night I tried a setting of 10-11 to see what the night would look like, and I woke up almost instantly feeling like the APAP was trying to clear an obstruction but wasn't succeeding very well, similar to waking up before CPAP feeling like I'd swallowed my tongue. For the very little sleep there was, all it showed was 3.0 flow limitation. So for my comfort level, I think I need to have the setting higher to keep from waking up with that feeling, and tonight I'm going to try a 10-12 range just to see how that works. Last night after putting the range back to 10-14, I did have .2 NR again, so I guess there's a trade-off there and I have to decide which way I want to go. I woke up with the feeling of obstruction; I didn't with the centrals and the big ol' string of apneas. So if rest is the goal, then I guess I go with the centrals, but it doesn't seem right that there should have to be a choice. Yeah, yeah. I know. Life isn't fair. I'm just trying to get through until the lovely PB arrives next week and find the right restful combination, elusive so far. I'm sure the DME will shit a brick when they print out my data this Friday -- I'm hoping they'll just be looking at compliance and won't notice. And, on that, I'm trying to cut a deal with them to trade out the M Series humidifer with a stand-alone and rent me a PB for after my loaner goes home. Until we see if what's going on with the centrals is enough to talk to the doc about a bilevel, if the insurance company is only going to buy one machine, then I want to make sure it's the right one since I'll be stuck with it for five years.
Here's the chart.

Peggy
Here's the chart.
Peggy
I have to say this surprised me. I tried a 10-12 range last night since most of the NRs have been in the 13 and 14 range. But lookie there! No snores in those places, either. So I've now had them at 11 and 12, too, and they definitely seem to correlate with a string of apneas. So I'm thinking they're not pressure related maybe as much as apnea related (score one for the doc) and so, rather than avoiding certain pressures hoping to avoid the centrals, we should be just trying to find the combination to get the lowest amount of apneas so they won't trigger the centrals. Right? Which is what you smart people have been trying to tell me all along, I think, but I am slow apparently. What the combination is, though, to get rid of the apneas enough to get rid of the centrals is beyond me.
Any suggestions? My lowest AHIs have been at the 10-14 range, although they've certainly run the gamut, and I'm having centrals regardless of lowering the range, so I'm thinking back to 10-14. What do you think?
Peggy
Any suggestions? My lowest AHIs have been at the 10-14 range, although they've certainly run the gamut, and I'm having centrals regardless of lowering the range, so I'm thinking back to 10-14. What do you think?
Peggy
For those curious to know how my 420E trial is going, I can report now three nights of use and one nap. (I don't know where my naps go, honestly. I thought I had one each day but can only find a report for one.)
Problem is here, friends, that I cannot figure out how to just get an average for you the way EncoreViewer does where it adds up all the different events and give you the AHI so will have to give you all the figures that it breaks down and leave it up to you to figure out what it means. I just am not getting this SilverLining software, I'm afraid, although I've at least learned how to save the .pat files and print the synthesis report for my book I keep.
Here goes. I'll give the hourly index numbers. I had this all nicely spaced so it would line up, but it's not cooperating with me; thus the periods for spacers. Sorry.
(First two days at 10-20 range.)
....................A..........A/CA........H.........H-FL.......AV........ 90%
5/12......... 1.4.......... 1.2........ 4.6........ .5........ 1.6........ 13
5/13 N........ .7.......... 1.4........ 0........... 0.......... 0......... 10
5/13........... .4........... .3........ 2.1......... .5......... 1.2....... 14
(Range now changed to initial 11, min. 10, max. 14)
5/14......... 1.2......... 0........ 1.3.......... 1.8......... 1.8........ 14
Now, what that all means, frankly I don't have a clue. I will leave it up to my CPAP gurus to interpret and lead, as always.
Peggy
Problem is here, friends, that I cannot figure out how to just get an average for you the way EncoreViewer does where it adds up all the different events and give you the AHI so will have to give you all the figures that it breaks down and leave it up to you to figure out what it means. I just am not getting this SilverLining software, I'm afraid, although I've at least learned how to save the .pat files and print the synthesis report for my book I keep.
Here goes. I'll give the hourly index numbers. I had this all nicely spaced so it would line up, but it's not cooperating with me; thus the periods for spacers. Sorry.
(First two days at 10-20 range.)
....................A..........A/CA........H.........H-FL.......AV........ 90%
5/12......... 1.4.......... 1.2........ 4.6........ .5........ 1.6........ 13
5/13 N........ .7.......... 1.4........ 0........... 0.......... 0......... 10
5/13........... .4........... .3........ 2.1......... .5......... 1.2....... 14
(Range now changed to initial 11, min. 10, max. 14)
5/14......... 1.2......... 0........ 1.3.......... 1.8......... 1.8........ 14
Now, what that all means, frankly I don't have a clue. I will leave it up to my CPAP gurus to interpret and lead, as always.
Peggy
-
Guest
NOTE: You NEED to forget the above "limit" settings suggestions when dealing with the 420e. Those suggestions were specific to the Remstar. Do NOT use them on your 420e.pjwalman wrote:So I think, Snoredog, that you are recommending I lower the maximum pressure to 11. And since I was having more events before when I had the lower pressures with the doc starting me at 6 (where I can hardly breathe, BTW), would a range of 8-11 be good do you think? Or could I even do a 9-11 or 10-11? I'd appreciate your input!
Peggy
I give suggestions based upon the machine you are using and how I know it functions algorithmically.
You cannot apply those principals on this different machine. The machine you had does a very poor job at differentiating the difference between a central apnea and obstructive. Some like to wing it and boast about that NRAH circuit but they are only fooling themselves. You no longer have that machine so forget those settings.
The 420e is a totally different animal, it will NOT respond to Central Apnea (CA) period. Remstar responds to event first then asks questions later, the result is it makes lots of mistakes. By the time it realizes this it is too late it already responded with pressure, so you cannot turn back the clock you grow some balls throw up a flag and instead of saying you made a mistake you claim it as a feature.
But it is commonly known if you respond to a CA with pressure it will most likely get worse. That NRAH circuit on the Remstar can be compared to gee I hit myself in the head with the hammer 6 times and it still hurts think I'll stop now. So if you "know" that you start getting hit with the hammer at 13cm pressure you avoid that pressure by imposing limits, that was what was done on my prior pressure suggestion.
SO now you have a 420e, it doesn't respond like a Remstar, it responds similarly to a Resmed but even better. So the suggestions I make from now on will be geared towards your particular disorder and the current machine.
NOTE: There is NO reason to "limit" the pressure on a 420E. If it says it is a Central it will log it as such on line 2 of the 96 hour report, you can pretty much be assured if it says it is a CA that it won't be responding to it with increased pressure, it will either maintain current pressure or drop but it certainly won't increase pressure.
Now, what you have is a form of obstructive apnea combined with a few centrals. Is it CSDB? I would say not, but it means you need a machine that better responds more accurately to the event seen and does NOT respond to events where same pressure makes the event worse. You may need 14 or 15 cm pressure at certain times and it may not fire off a CA at all. Other times they may start firing off at 8.0 cm pressure.
Basically, you need a machine like the 420e that does a better job at differentiating the difference between a central and obstructive event. You want it to "respond" to obstructive events seen and "avoid" any response to Central Apnea seen.
However, the 420e was designed to function with a wide variety of patient needs and the default settings of the machine reflect that.
Based upon the events seen in your case (CA patterns seen), you may need to "tweak" the 420e so it better responds and/or more precisely to your particular need.
Minimum or Initial pressure:
You always want the machine watching for events and NOT blindly responding to them like what happens when you use CPAP pressure or use a Minimum pressure set up "high". Toss out that set Minimum to CPAP titration theory as it does nothing in your case. You have CA at all different pressures, worst thing you can do is "hinder" the machine in early detection of those pre-curser events by using a Minimum pressure set up too high. For the first few weeks, have some faith in that little machine, it does a fine job if you allow it to.
Based upon what I seen above from the 420e data, you need to:
1. Increase the Max to 20 cm, there is absolutely no reason to be limiting the max pressure on the 420e.
2. Lower (yes I said lower) the Initial pressure from 11 down to 8.0. Allow the A10 parameter to work. If you have insomnia or cannot get to sleep due to machine noise/pressure etc. then set up the Ramp with even a lower pressure but no lower than 6.5. Use this during those nights you may awaken and find pressure to be annoying. Set the timer for 30 minutes.
3. Disable IFL1: This is "Command on Flow Limitation" setting, enabled the machine is aggressively responds to Flow Limitation. In your case you don't want that happening, you only want it responding to FL when it is associated with a Hypopnea (handled by IFL2 setting, leave that one checked).
4. After disabling by unchecking the IFL1 box, compare your reports, you should see the pressure sine wave change, it should have more sharp peaks and valleys compared to stairs or rolling hills. This means if the machine sees an apnea it will increase pressure to eliminate it, then drop back down faster so said pressure doesn't aggravate the condition that leads to more CA's. Your goal is to have NO CA's during the night. With a few tweaks on the machine you should be able to achieve that.
5. IF the CA's do not reduce then you may have to change the default pressure the machine uses to avoid response to CA when it cannot determine if an open airway exists. This is called "Command on Anea" or A10 parameter. By default it is set to 10 cm pressure. In your case you may need to lower it (never increase it), because your threshold for CA appearing may be lower than the industry standard of 10 cm pressure, we are human beings so you may not follow the status quo for that standard. If the CA's don't start lowering with the above settings you would slide the A10 parameter from current 10 to 9 and observe a few nights reports. Again, you are trying to stablize sleep so CA's return to zero. In its CA detection, the 420e listens for an open airway which allows it to hear your cardiac oscillations, kind goes back to the 2 cans and string theory from when we were kids. Those cardiac oscillations heard from an "open" airway is how the 420e it determines if the event is central or not. The Remstar and the Resmed don't do that or at least they don't advertise they do that. Remstar relies on that NRAH circuit and Resmed its patented A10. Now, not all CA's have an open airway (only about 60% do), the others may be closed, in the case of a closed airway, the 420e uses that A10 parameter to decide if it should respond with pressure (by having your Minimum set to 11 you are effectively "masking" that parameter OUT or disabling it where it does NOT function, reason to lower your Initial pressure back to 8.0).
If there is anyone that is conservative with machine pressure settings it is me, but don't hinder the machine from making decisions on its own by use of incorrect settings or following bad advise meant for CPAP.
IF you have plain jane run of the mill obstructive sleep apnea you can set it up like a cpap machine and get by with doing that. But you don't have run of the mill OSA it is complicated by centrals so it requires a bit more care in machine selection and setting it up correctly so it responds to your particular needs.
So based upon what I have seen, I would set your 420e up as follows:
Minimum pressure=8.0
Initial pressure=8.0
Max pressure=20
A10=10 (default command on Apnea setting)
IFL1=Disabled (unchecked, default=checked)
IFL2=Enabled (checked, default=checked)
IF CA's persist on line 2 after you set to above, you may need to lower A10 from current default 10 cm to 9.0 cm, this changes the way the machine responds based upon current delivery pressure. Basically it forces machine to watch for CA's at a lower pressure threshold when Cardiac Oscillations from an open airway are NOT seen indicating the event may be obstructive. This parameter is only used when no cardiac oscillation can be heard. So it says if current pressure is 10 or below and no cardiac oscillations are heard, apply pressure as the event is obstructive. If current pressure is OVER A10 or 10 cm and no cardiac oscillation are heard then it won't respond to the apnea for fear it may be central possibly with a closed airway such as with a mixed apnea, then it looks at pre-curser events like snoring to help decide if it should increase pressure or remain.
Low pressure can be your friend use it.
oops that was me,
Note: on your Remstar report NR's, those central apnea can be post arousal centrals, meaning they show up after an arousal from an obstructive event. SAG once had a EEG graph showing that. How does that differ from say a "Mixed" apnea? That is a question for SAG but my guess is they are similar.
The CA you are experiencing are random and show up at any pressure most likely even at constant CPAP pressure (if you had a way to see them).
So even with straight CPAP pressure set to where you "think" it would address all possible obstructive events you could still find yourself waking in the middle of the night after your fight or flight response kicked in to start you breathing again. This is why even straight CPAP or many autopaps may not work for you.
Again you need a machine that better differentiates a central from obstructive apnea and is able to "respond" above any conventional command on apnea hard coded setting yet avoids responding to centrals.
Your 420e is just that machine, it WILL respond to frank apnea above 10 cm pressure unlike the Resmed and even the Remstar but it does so more accurately.
So if you need 14cm pressure to splint an obstructive apnea, your 420e can still do that and also avoid responding to a central at the same time.
Note: on your Remstar report NR's, those central apnea can be post arousal centrals, meaning they show up after an arousal from an obstructive event. SAG once had a EEG graph showing that. How does that differ from say a "Mixed" apnea? That is a question for SAG but my guess is they are similar.
The CA you are experiencing are random and show up at any pressure most likely even at constant CPAP pressure (if you had a way to see them).
So even with straight CPAP pressure set to where you "think" it would address all possible obstructive events you could still find yourself waking in the middle of the night after your fight or flight response kicked in to start you breathing again. This is why even straight CPAP or many autopaps may not work for you.
Again you need a machine that better differentiates a central from obstructive apnea and is able to "respond" above any conventional command on apnea hard coded setting yet avoids responding to centrals.
Your 420e is just that machine, it WILL respond to frank apnea above 10 cm pressure unlike the Resmed and even the Remstar but it does so more accurately.
So if you need 14cm pressure to splint an obstructive apnea, your 420e can still do that and also avoid responding to a central at the same time.
someday science will catch up to what I'm saying...
Thank you, SnoreDog. I appreciate your input! Wow! I know *my* brain wouldn't be up to the task -- thank goodness I have the brains of you all to pick!!!
I may have another machine decision to make soon. I have faxed my doc to ask him to authorize a BiPAP Auto trial because I am still fighting a losing battle with aerophagia and getting kind of discouraged about it, even sleeping without the CPAP sometimes now, which is something I refused to give in to at the start.
So we'll see what happens with that. Otherwise, my new DME carries Respironics -- big surprise -- and I'll be going back to the M Series, looks like, although I won't be taking the financial hit I did with the previous DME.
Thanks again!
Peggy
I may have another machine decision to make soon. I have faxed my doc to ask him to authorize a BiPAP Auto trial because I am still fighting a losing battle with aerophagia and getting kind of discouraged about it, even sleeping without the CPAP sometimes now, which is something I refused to give in to at the start.
So we'll see what happens with that. Otherwise, my new DME carries Respironics -- big surprise -- and I'll be going back to the M Series, looks like, although I won't be taking the financial hit I did with the previous DME.
Thanks again!
Peggy
Aerophagia is another reason to keep that Initial pressure lower, using 8.0 or even 7 will help with that.pjwalman wrote:Thank you, SnoreDog. I appreciate your input! Wow! I know *my* brain wouldn't be up to the task -- thank goodness I have the brains of you all to pick!!!
I may have another machine decision to make soon. I have faxed my doc to ask him to authorize a BiPAP Auto trial because I am still fighting a losing battle with aerophagia and getting kind of discouraged about it, even sleeping without the CPAP sometimes now, which is something I refused to give in to at the start.
So we'll see what happens with that. Otherwise, my new DME carries Respironics -- big surprise -- and I'll be going back to the M Series, looks like, although I won't be taking the financial hit I did with the previous DME.
Thanks again!
Peggy
Note: Pay special attention to humidifier settings, do NOT use the heat if ambient temp is high, too much humidifier can cause congestion and make it more difficult to breathe at lower pressure settings as you indicated a problem in the past.
Was it the lower pressure or was it too much humidification?
I don't ever use the heat on my humidifier at all, don't know why I keep buying humidifiers with the machine, I can get by with just the tank from a HC150, those are dirt cheap, in fact the one I have came with my manometer from cpap.com.
Maybe I'll make a oak board "holder" for it to keep the tank from moving around, that is all I need for a humidifier.
As for the bipap? Hopefully it will work, but bilevel can sometimes make centrals seen worse and in some cases even contradicted.
someday science will catch up to what I'm saying...