StillAnotherGuest wrote:split_city wrote:When upright, Pes at FRC is negative due to the elastic recoil of the lungs.
The effect, if any, of the elastic recoil of the lungs would be reflected as positive in
Pes.
I'm still a bit rusty when it comes to compliance, elastic recoil etc. In simple terms, FRC is the
lung volume at which the outward recoil of the chest is equal and opposite to the inward recoil of the
lung. Why is Pes negative at FRC? To understand why, I simply use an airfilled syringe. Please correct me if I'm wrong as this isn't my area, but I would love to learn. Think of the inside of the syringe as the lungs or esophagus while your hand represents the ribcage. Put your finger on top of the syringe and pull the plunger down and hold the plunger in place. Say this point is analagous to FRC i.e. the inward recoil (syringe/lungs) is balanced by the outward pull on the syringe (hand/chest). If you let go of the syringe, the syringe would recoil back. If you measure the pressure inside the syringe when you held the plunger in place, the value would be negative i.e. what it would be in the lungs at FRC.
StillAnotherGuest wrote:split_city wrote:However, it's generally positive when an individual is in the supine position because medialstinal structures compress the oesophagus, thus compressing the oesophageal balloon. Most of my baseline values have been between 5-10cmH20.
For those patients, you're going to have to account for that as artifact. That's not a respiratory variable.
Yep, I understand that this positive value is an artifact. Unfortunately, we cannot measure pleural pressure.
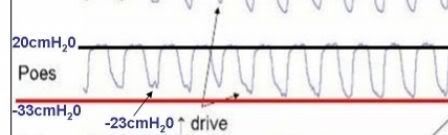
StillAnotherGuest wrote: split_city wrote:Now, the 20cmH20 you are seeing is at peak expiration, not FRC. You would expect Pes to go up a bit...
A bit yes. 20, no.
Ok, I have had a look at some other data from some of my other patients. During basal breathing when 1) drive is low and 2) no increase in Pga during expiration, peak Pes is around 5-10cmH20. However, patients with increased drive + Pga increases during expiration, had a peak Pes between 15-20cmH20. The patient with the 20cmH20 peak in Pes during high drive situations, only had a peak of around 10cmH20 during breaths under low drive conditions.
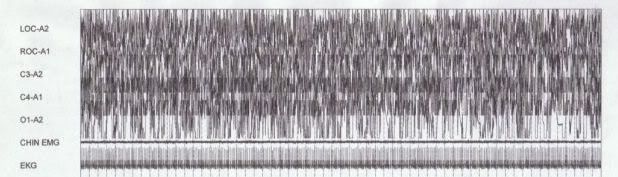
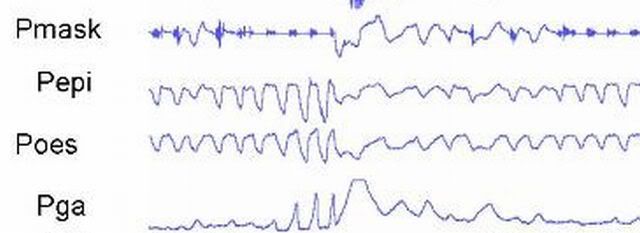
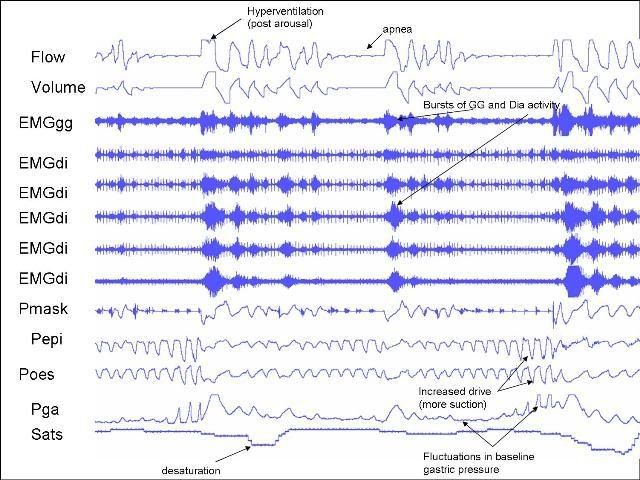
StillAnotherGuest wrote: split_city wrote:However, as I said previously, drive was increased in this patient. This drive was transmitted to to abdominal muscles. These muscles are generally pretty silent during "normal" breathing. However, they tend to crank up during increased drive and contract during expiration. You can tell this to be the case because gastric pressure was increasing during expiration (towards the end of the apneas) in my very first picture I put up. This increased contraction of the abdominal muscles during expiration also contributes to the raised expiratory Pes.
The first screen
is more representative of
Pes. A
transient increase in
Pes activity (as well as
transient gastric pressure elevation during response to apnea)
Ok, I won't draw them on the picture but this guy's peak Pes during his obstructive events (times when drive was high and Pga increased during expiration) was also between 15-20cmH20. His peak Pes during low drive conditions was around 5-8cmH20
StillAnotherGuest wrote:But this guy
is very aggressively performing
active exhalation (+20 cmH2O) even during periods of "baseline" breathing. He'd need an enormous
Pcrit to have to do that, which would make him an "obstructed airway" patient rather than an "OSA" patient.
Again, this is during a high drive state and hardly constitutes "baseline" conditions i.e. patent airway. His airway is acting as a starling resistor. His GG is active enough to prevent a full on obstructive event. Unfortunately, the Pga trace was lost during this period but I would bet he was cranking his abdominal muscles, thus increasing Pga, during this high drive state.
As I have pointed out, he wasn't the only one to show a peak Pes of around +20cmH20 during these high drive conditions.