Some simple comments on BiLevel function & Exhale Relief function. (#2 - this post has actually turned into a bit of a history lesson - just rolled out that way)
If we start with CPAP of which the 1st commercial machine was (IIRC) a Sullivan model (later renamed Resmed). But the first exhale relief introduced was the Respironics BiLevel. They coined the name (trade marked) BiPap and very quickly after that Healthdyne came out with a BiLevel (aptly called a BiLevel). Then came (IIRC0 The Sullivam and the early Puritan Bennett plus some other BiLevels).
BiLevels were
very very expensive and thus were only made available to people with COPD or other lung problems. In the early days they still had not come up with a CPAP / BiPAP that could deal with centrals.
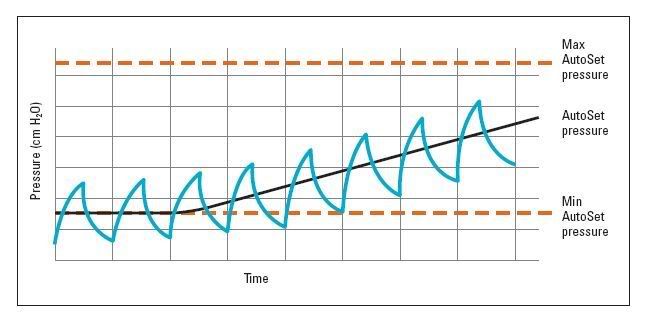
Next Resmed came up with an advanced concept for adjusting the pressure automatically (The Autoset). The purpose here was to keep the machine at as low a pressure as needed as this helped keep away from pressures that had too many negative side effects.
At approx the same time Respironics added timed mode to their BiPap (this was still the big square box model). This became known as the BiPap S/T (Synchronous and Timed), this machine was then applied to people with centrals.
The Sullivan BiLevel & the Puritan Bennett BiLevels also added timed mode.
All BiLevels then began to add ways to adjust the rise & fall time (the speed with which the machine went from Epap to Ipap (rise) & Ipap to Epap (fall). In particular, people were finding that it was a strain on them and disruptive to sleep if the risetime transition from Breath-out to Breath-in happened too quickly.
Healthdyne and Respironics also entered the market with Autos (this period was the late 1990s).
Then Respironics adopted the approach of using software to determine the difference between leaks and breathing - this algorithm was in the feature they call Auto-Trak. The other vendors took the approach of mainaining leak rate tables in the software inside the machines to determine what was leak vs breathing. The Auto-trak approach offers more flexibility because it can adapt to different masks but the Resmed / Puritan Bennett approach was much more accurate but does require the machine to be set for the correct mask. Resmed added an Auto-trak equivalent but called it V-Synch.
Leak vs breathing accuracy is really important in a BiLevel because of the need to get the Ipap to Epap to Ipap transitions correct. A machine that has difficulty detecting slow breathing vs a leak will get its timing wrong.
Then Respironics introduced an innovation into its Cpap and Auto models & called it C-Flex, it was an extension of the Auto-trak algorithm & so on top of the machine being an Auto (which gives relief by keeping pressures as low as it can based on the settings) there was this exhale relief that could be set to 3 different settings.
At this same time Resmed and Puritan Bennett began adding more adjustments to their BiLevels as many more side effects were emerging.
One significant problem was that if the Ipap pressure was higher than it needed to be and the gap to Epap was too great, people could begin to hyper-ventilate & that disrupted sleep. Respironics BiPap machines had less rise/fall adjustments that the other brads but solved that issue by adding the Bi-Flex feature. BiFlex provides a dip to the Ipap & Epap pressures as the users transitions from one mode to the other. This kept their machines simple & easier to adjust by non-technical users. For example, it takes some expertise to set up a BiLevel & the PB330 is a classic example of that complexity.
Respironics then came out with an innovative Auto BiLevel that sought to keep the gap to a minimum (2 CMS) and to adjust the Ipap and Epap independently. This idea was very innovative for the time but there is insufficient research to know if this has improved use of BiLevels or created some new issues.
Resmed then took the concept of a BiLevel, came up with what they considered optimum rise time & created EPR. EPR offered the equivalent of a BiLevel that could be adjusted for a 1, 2 or 3 CMS Ipap to Epap gap. This is very adequate for the non COPD user.
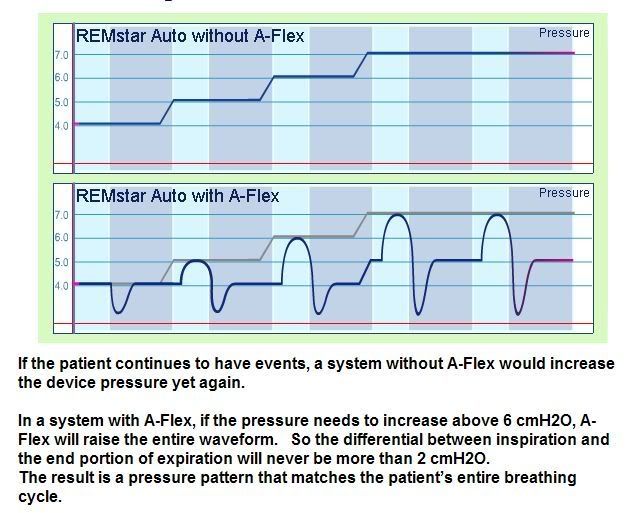
Respironics continued their innovation by adding another feature to their Auto called A-Flex. This feature took the basic C-Flex function (exhalation relief) and extended the pressure control into the breath-in part of the cycle. This solved an issue with C-Flex where as C-Flex ends, there is a sudden rush of air as full pressure resumed. This rush if C-Flex was set high (3) could cause mouth popping (pops of air escaping) or bubles going into the stomach (aerophagia). A-Flex was intended to solve that. It also acts as a sort of a BiLevel in that the machine keeps the A-Flex min max pressure gap to max 2 CMS.
As has been happening lately, the next generation of Servo Ventilation machines appeared 1st with the Resmed Vpap Adapt and now the Bipap SV.
These machines push the technology to new limits but already are showing they can provide results that are the best hoped for. They provide the best type of relief to people on CPAP therapy but because they are still in their early days are mainly being supplied to people with disorders such as Cheynes-Stokes breathing or Central-Apnea or Complex-Apnea
But make no mistake, the SV type machines are the future & as costs come down expect to see our garden variety CPAPs looking more like them.
For me, I admire the innovation of all the companies involved. There are some very dedicated & smart people working hard to make our lives better.
DSM
PS Anyone please feel free to correct any point - it is a lot of history & may be out of seq or important bits left out or given a wrong emphasis.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition):
respironics,
resmed,
bipap,
Puritan Bennett,
C-FLEX,
CPAP,
auto
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition):
respironics,
resmed,
bipap,
Puritan Bennett,
C-FLEX,
CPAP,
auto