




APAP Discussion




You can take SAG's quotes and play them back over and over and they don't apply in every case. you guys seem to be bundling CSDB and central apnea in the same category which it is not. Central apnea can occur without any cpap machine in the picture at all, such as the case with myself and bluegrassfan, frequenseeker and many others I've seen come by here. With CSDB the apnea condition gets worse on cpap.rested gal wrote:Snoredog, you've done a lot of experimenting with a lot of machines while working on your own treatment. The type of sleep disordered breathing that showed up on your PSG happened to involve a lot of centrals for you. Your lab titration and your own use of autopaps found what's right for you. I don't know this for a fact, but my guess is that your case is rather unusual compared to the type of sleep disordered breathing most people have.
If that Mayo study is right, approximately 85% don't have the kind of SDB problem that may be what was revealed in your PSG sleep study, Snoredog...i.e. the numerous centrals you had along with your other OSA events. The experience you have when you increase pressure is not likely to happen to most people with plain OSA who choose to use an autopap, imho. I think your own experience very much colors your advice about autopap settings. But then, that's probably so to one extent or another for all of us.StillAnotherGuest wrote:Morgenthaler et al at Mayo in Complex Sleep Apnea Syndrome: Is It a Unique Clinical Syndrome? in SLEEP 2006:9 showed that the incidence of CompSAS (which would pretty much be the thing that would get you into trouble with pressure-induced events) was about 15%, so that might be a good number to start with.
SAG
I do think that your insistence on the danger of raising pressure and risking "pressure induced centrals" is overstating the possibility because you've seen that happen to you. I don't think that would happen to most people using autopap. Just my opinion, and I'm not a doctor.
viewtopic.php?t=14225
Page 2:(bold emphasis mine)StillAnotherGuest wrote:The phenomena of pressure-induced central apneas is tossed around far too freely. The vast majority of people do not get centrals because of ultra-therapeutic CPAP levels. BiLevel, Pressure Support (PSV) and Proportional Assist (PAV) Ventilation are another matter. You need some mechanism to drive the pCO2 below the sleeping apneic threshold, and plain old CPAP rarely is able to do that. OK, if you wanna argue that CPAP increases base lung volume (Functional Residual Capacity)(FRC), and since that increases gas exchange, some people can generate centrals that way, fine. But it's not as many as you might think.
SAG
True, SAG was referring to "plain old CPAP", not autopaps. However, I think autopaps are delivering one straight cpap pressure, too...varying that pressure, yes. But I think autopaps are more in the category of "CPAP" than being the type of machines that would deliver the kind of treatment (BiLevel, PSV, PAV) he goes on to speak of as being "another matter."
For bluegrassfan his CA dropped from 22 to 2 which after cpap which is actually good considering CA doesn't usually respond at all to cpap pressure, that is why it is so difficult to treat with conventional therapy. But that was only one night's data, he will have no idea what is happening to those CA's once he leaves the lab. Do they get better or do they get worse?
Even if he selected the PB 420E like the report SAG posted above, PB themselves admit that the 420e can only detect or differentiate central apnea 66% of the time even on a good day. That means 6-7 out of 10 is the best the 420e can differentiate and it is one of the better autopaps at detecting them. Now look at how many Apnea/CA's Wally had in that report above. I count quite a few, if I had to guess there is a apnea along with those CA's so some of those are probably Mixed apnea.
While our disorder may share some of the same characteristics of CSDB such as residual fatigue, I don't consider myself as having CSDB. CSDB gets worse going on cpap and can be influenced by pCO2 rates which was what the first study done by Harvard was about. In that study they played more with masks using more dead space and retained more CO2 to manipulate the therapy. I thought it was ingenious, they were faking out the respiratory drive using a special mask and using a machine which better avoided the CA events. So if they manipulated the respiratory drive correctly CA subsided.
You guys seem to insinuate the condition is very rare, I'd consider 2% being rare, CSDB may be rare and only 15% of the population as the Mayo study suggests from the 233 patients it had studied, that is still what 35 patients out of the study.
CG can make all the don't flame me disclaimers she wants then goes ahead and stirs the chili, it is obvious to me that CG directed her comments in #5 directly at me since I'm the only one here that has the balls to discuss it. Like I said she doesn't have a clue about the disorder so as far as she is concerned it is totally without merit.
Take 100 patients, put them in a lab titration setting, use SAG or anyone you want, start titrating them from 5cm and continue to increase to 20cm then count up the number of patients that blew CA's, I'll bet you there are a lot more than just 15 out of those 100. Your diagnostic PSG can show 0 (zero) CA's then when you apply cpap pressure they can show up (or not show up).
Ask SAG what terminates a titration study. He'll tell you, when the obstructive events subside and good sleep is obtained. But if the patient snores, they may try to also eliminate those snores and in doing so they can cause a central which wakes the patient, from the pressure being too high. Once the patient is awake the study is pretty much over. Autopap machine is not that good, it ain't gonna stop until the snores go away.
Autopap does the same thing, it will also chase those snores and it too can blow the central just like the lab tech can manually. Difference is the lab tech can see them, the autopap cannot. Once you leave the lab you are totally blind and can't see them either.
I'd sure hate to be a Kaiser patient in this day and age, no diagnostic PSG, just send them home with an autopap for a week set from 4cm to 20cm, bring them back and give them the cheapest machine available. According to the Mayo numbers, that means 15 out of 100 Kaiser patients are at risk of CSDB or centrals apnea and will have no idea they have the condition or what they should be avoiding. All just to pad the coffers of Kaiser and its investors.
Look at Wally's 420E report above that SAG posted, he was set 4cm to 20cm, and sure enough he went all the way to the top at 20cm. He was still snoring when his head rung the bell at 20cm pressure and still having FL's. Guess what, his snoring doesn't stop with cpap pressure increase no matter how high it goes, nearly all the autopaps trigger on snores even when they don't respond to apnea over 10cm, they will still respond to snores. It would be nice if you could set a parameter to prevent a machine from responding to snores over a certain pressure. Maybe someday.
Patients that have the disorder described as CSDB may be in deed rare, those that have CA due to too much pressure are not as rare in my opinion.
Maybe we should do a poll here using 100 members, have them drag out their PSG and indicate weather or not they had CA denoted on their diagnostic PSG.
When ever I see someone show up here with CA's in their PSG report, they snore and their pressure is only 8-10cm (usually it is only 8 to 9cm), I assume that pressure is there for a specific reason especially if snores continue and are noted on the titration report. It says to me this patient has CA, we tried to titrate them to get them below AHI=5 but they continued to snore but when we increased pressure CA's increased as well. So we settled back down below 9cm pressure where best sleep was obtained. Let them snore!, trying to eliminate them only increases the frequency of the CA's. Most patients NEVER get this information.
Ah man, 9cm is so hard to tolerate, they show up here, first suggestion, lab missed your titration, you need a Autopap.
Sure enough, they order it, it shows up plug it in leave it at default 4cm to 20cm range as set by some genius RT, machine sees those snores then blows the top of their heads off and they wonder why. Seen it a hundred times here.
The whole concept here is how you set up the machine. You can set it up so that it finds a new pressure or you set it up so it avoids causing a problem. I prefer to error on the conservative side.
-
StillAnotherGuest

- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
Anonymity?
Although SAG generally prefers to play "Panama" by Van Halen repeatedly.Snoredog wrote:You can take SAG's quotes and play them back over and over
This is perhaps the most important point of the half dozen concepts here. Are you better, worse or the same. The large scale study of the effects of CPAP on CHF/CSA in CANPAP showed that CPAP actually dropped the AHI by half (40 to 21). Maybe not the best, but certainly better. And if you wanna say pressure therapy generates centrals, then there has to be a bunch, like a burst at an AHI rate of 40-60 because the cascade is set in motion and each central will force another. All these guys that go "Omigod, a central apnea, it's the apocalypse!!!" need to take some venlafaxine (no, no, don't do that, only kidding!!). The relationship of isolated CA during aggressive pressure titration is often as a result of arousal (high pressure aggravates patient, he then has arousal, briefly hyperventilates, has compensatory CA (which makes it a NORMAL response) and returns to baseline).you guys seem to be bundling CSDB and central apnea in the same category which it is not....With CSDB the apnea condition gets worse on cpap.
Right, but they claim 100% sensitivity for all apneas, so we can still get a clue.PB themselves admit that the 420e can only detect or differentiate central apnea 66% of the time even on a good day.
That ain't Wally. Wally's much taller...look at how many Apnea/CA's Wally had in that report above.
You would have been right.if I had to guess there is a apnea along with those CA's so some of those are probably Mixed apnea.
To illustrate that point, these guys noted that the number jumps to 28%:RG said that SAG said that SAG read... wrote:The phenomena of pressure-induced central apneas is tossed around far too freely. The vast majority of people do not get centrals because of ultra-therapeutic CPAP levels. BiLevel, Pressure Support (PSV) and Proportional Assist (PAV) Ventilation are another matter. You need some mechanism to drive the pCO2 below the sleeping apneic threshold, and plain old CPAP rarely is able to do that.
Bilevel Positive Airway Pressure Worsens Central Apneas During Sleep
Right, that's the fine line. But you do have to address the snoring, and if it's generating arousals you are obligated to attack it. SAG shoots techs who leave residual snoring in titrations.Ask SAG what terminates a titration study. He'll tell you, when the obstructive events subside and good sleep is obtained. But if the patient snores, they may try to also eliminate those snores and in doing so they can cause a central which wakes the patient, from the pressure being too high.
The above APAP disaster was actually set up by some genius DME RT. Seems like I'm always fixing their botched mess of pseduo-medical trickery (pseduo?).Sure enough, they order it, it shows up plug it in leave it at default 4cm to 20cm range as set by some genius RT
Oh God, I'm turning into Snoredog. During Lent, no less.
Perhaps SAG will post as "Black Bart" so he can fire off personal barbs, since he is unfortunately aware that the mudslinging threads get about 7 to 10 times more views than the more civil posts. This way he can remain anonymous.
LOUD THUNDER CLAP, BLINDING LIGHTNING BOLT
Or not.
SAG

Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
NightHawkeye

- Posts: 2431
- Joined: Thu Dec 29, 2005 11:55 am
- Location: Iowa - The Hawkeye State
Re: Anonymity?
Nonsense, SAG. Every time I see a SAG posting, I immediately jump to it. The combination of sage wisdom, humor, and detailed guidance you offer is as good as it gets on this forum. You serve as an inspiration for aspiration.StillAnotherGuest wrote:Perhaps SAG will post as "Black Bart" so he can fire off personal barbs, since he is unfortunately aware that the mudslinging threads get about 7 to 10 times more views than the more civil posts.
Regards,
Bill ( . . . sincere apologies for the final pun, but I couldn't resist . . . )

Re: Anonymity?
StillAnotherGuest wrote: Seems like I'm always fixing their botched mess of pseduo-medical trickery (pseduo?).
OMG!!!.....Look everybody!.....The genius DME RT can't even spell pseudo. God!! He's dumber than dirt.........IT'S CALLED A TYPO!!! Get over it.
Seems like I've somehow upset the Polysom. Techs. here on the forum. I am truly sorry. I suppose it took me a little while to learn how to act on this forum. Therefore, I'll try to stick to having 'Ivory Tower' medical discussions amongst ourselves so the average PAPer will have to Google our every other word and make ourselves look like Gods here on the forum. Because, when it comes right down to it, it's all about how many polysyllabic, latin rooted words that I know.
DISCLAIMER--The above poster is not a professional comedian. He is a medical professional. Any attempt to construe the above as humorous is soley at the reader's discretion. The poster is not responsible for any laughs, explicit or inferred. Your mileage may vary. Tax, tags, and title not included. Have a good day and a better night!
To know even one life has breathed easier because you lived. This is to have succeeded. -- Ralph Waldo Emerson

Re: APAP Discussion
StillAnotherGuest wrote:It happens a great deal more than you think.
SAG
Well, yeah, I was, kinda. My first titration study I only slept 42 minutes the entire night.BrianRT wrote:ummmm......I 'THINK' it nevers happens in my dealings with sleep labs. IF it does, then GREAT, it SHOULD be the default, instead of the exception. My point is, a number of sleep labs use auto's as their 'go-to' device when they can't properly titrate (*gasp* dirty insider secret just leaked folks...no pun intended). Problem is, the patient has to pay for that 2nd night titration study when NOTHING WAS ACCOMPLISHED.
But, if it happens 'a great deal more than I think', then let me ask the opinions of the residents of this fine forum. Has anyone ever been told to come back for another titration study because the lab couldn't quite get it right the first time??
I was aware thru these apnea forums that Medicare REQUIRES AT LEAST 2 hours sleep out of 6 hours of "sleep (or bed) time". So I was on the phone immediately w/the sleep lab manager when I got home yet that morning to tell her that I considered the titration study inadequate and was aware that Medicare required 2 hours of sleep, etc., etc., etc.
I was assured the intent was to call me back in for another titration study. Whether I totally buy that or not, I'm still not sure. But the fact remains, I like my sleep lab, sleep pulmo and all the staff so I choose to not dwell on it. They've always been very helpful and supportive and have gone to bat for me w/my sh*tty DME a couple of times.
I was scheduled immediately for the second titration study. I only slept 98 minutes the entire night of my second titration study. But 42 and 98 equal more than 120 minutes so I "qualified" for xPAP. Medicare was billed for both titrations but I don't remember if they were billed at 1/2 price or what, I would have to double check.
_________________
| Mask: Quattro™ FX Full Face CPAP Mask with Headgear |
| Additional Comments: PR SystemOne BPAP Auto w/Bi-Flex & Humidifier - EncorePro 2.2 Software - Contec CMS-50D+ Oximeter - Respironics EverFlo Q Concentrator |
Women are Angels. And when someone breaks our wings, we simply continue to fly.....on a broomstick. We are flexible like that.
My computer says I need to upgrade my brain to be compatible with its new software.
My computer says I need to upgrade my brain to be compatible with its new software.
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
You keep implying that even some harmless, "normal" centrals mean DANGER!! And that the instant even one central shows up during the course of some peoples' sleep lab titrations, it's a big deal. Both christinequilts (who DOES have Central Sleep Apnea) and StillAnotherGuest (also as "sleepydave") have explained many times that there can be perfectly normal ways that central apneas can happen -- asleep or awake. Even in perfectly normal people that have no OSA or any kind of sleep disordered breathing at all.Snoredog wrote:Take 100 patients, put them in a lab titration setting, use SAG or anyone you want, start titrating them from 5cm and continue to increase to 20cm then count up the number of patients that blew CA's, I'll bet you there are a lot more than just 15 out of those 100. Your diagnostic PSG can show 0 (zero) CA's then when you apply cpap pressure they can show up (or not show up).
You can dismiss quoting SAG all you want, but do read this again carefully:
(bold emphasis mine)StillAnotherGuest wrote:All these guys that go "Omigod, a central apnea, it's the apocalypse!!!" need to take some venlafaxine (no, no, don't do that, only kidding!!). The relationship of isolated CA during aggressive pressure titration is often as a result of arousal (high pressure aggravates patient, he then has arousal, briefly hyperventilates, has compensatory CA (which makes it a NORMAL response) and returns to baseline).
Perhaps it's the physical feeling of the change in pressure that annoys the sleeper and causes the arousal, more so than the higher pressure in and of itself. Whatever the mechanism, the point is that the central apnea that popped up at that point during the titration is a temporary thing. It's not necessarily an indication that THAT particular higher pressure is going to cause centrals from then on.
I think a point College Girl was making in her initial post in this thread (and a point I very much agree with) is that there's an exaggerated fear passed along regularly on the message board about the risk (small, in my opinion, for MOST people) of causing something -- "pressure induced centrals" -- if you raise the pressure setting on a cpap or autopap.
And even more unfounded fears are promoted about what a few centrals mean... for most people, anyway. Or that a central apnea is an especially dangerous thing...talked about as if it were more threatening than an obstructive apnea.
There's just something about hearing that a central apnea means the brain didn't send a timely signal, ("Hey, breathe.") that makes people think, "OMG, my brain FORGOT something like that! What if my brain NEVER finally remembers!!!" Really scares people unduly, imho.
We don't get alarmed about seeing that our AHI for the night was 3.0, meaning that some apneas and or hypopneas sneaked through. But the thought of even ONE central happening or a few centrals....OMG!!! An exaggerated fear, imho. (I'm not a doctor.)
Either way, obstructive apnea or central apnea, the BRAIN is what finally has to arouse us to breathe. The BRAIN has to wake up enough to send a signal to correct EITHER one.
We're lucky that OSA is the most common form of sleep disordered breathing. And that cpap machines can take up the slack (so to speak ) to keep the airway open.
All that said, I do understand that your own SDB is different from the plain OSA that most people have, Snoredog. You did have a lot of centrals in your diagnostic sleep study. So you do keep a closer watch, and rightly so, on what happens for you. You express strong objections to the kind of autopap settings suggestions that would not work well for you. I just don't think most other people would have the kind of problems you would have with a high ceiling for the top pressure setting in an autopap.
If what happens for you when you raise your upper pressure was a problem for most people, I think long before now doctors would have stopped sending people home for additional auto-titrating with a range set 4 - 20.
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Re: APAP Discussion
Just checking to see how the consensus is shaping up...On the Subject of APAPs CollegeGirl wrote: I think we need to at least try to come to some sort of general consensus on things... (If that's even possible).
Just chiding you, College Girl. But this certainly has been a very interesting thread so far! Put me down as one who also prefers and appreciates civility. There's absolutely no reason that differing opinions can't be exchanged without subtle or overt insults.
We get beat up enough by apnea without having to beat up on each other in threads about apnea. I hope this good discussion continues. And I hope this good discussion continues to stay civil.
Kudos to the thoughtful, courteous posters contributing to this thread!
-
rested gal
- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
If you're referring to the PB420E graph on page 2, I still wish I could'a sneaked in there to flip off IFL1.StillAnotherGuest wrote:The above APAP disaster
Might not have made one bit of difference for Wally. Oh, wait, you said that wasn't Wally??? I could have sworn the peaks looked tall enough to be him!
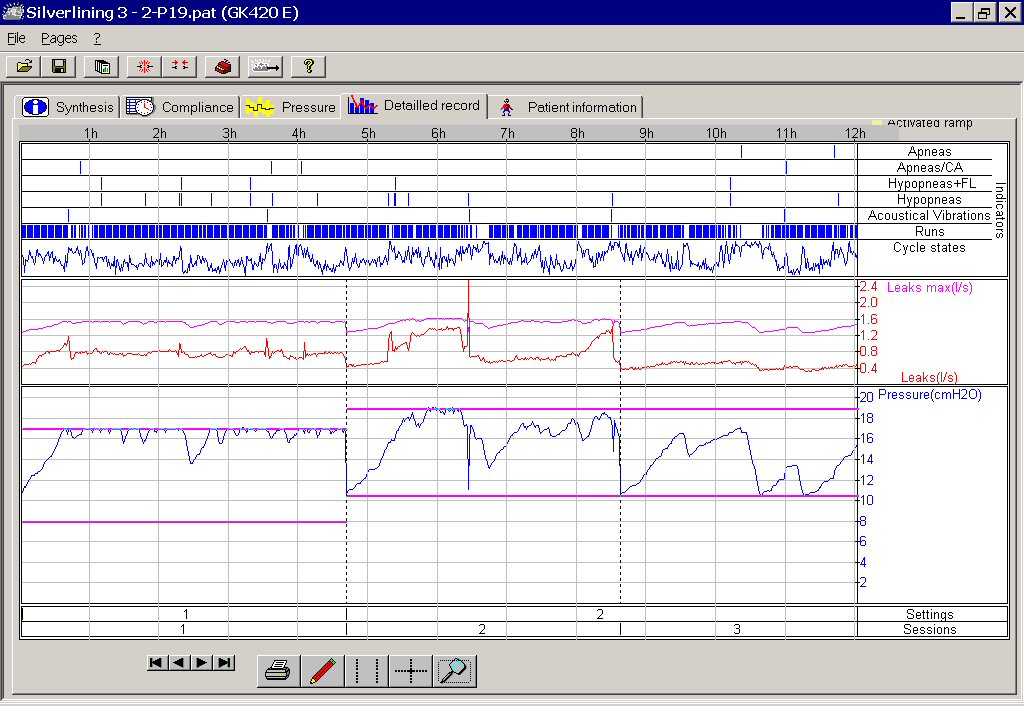
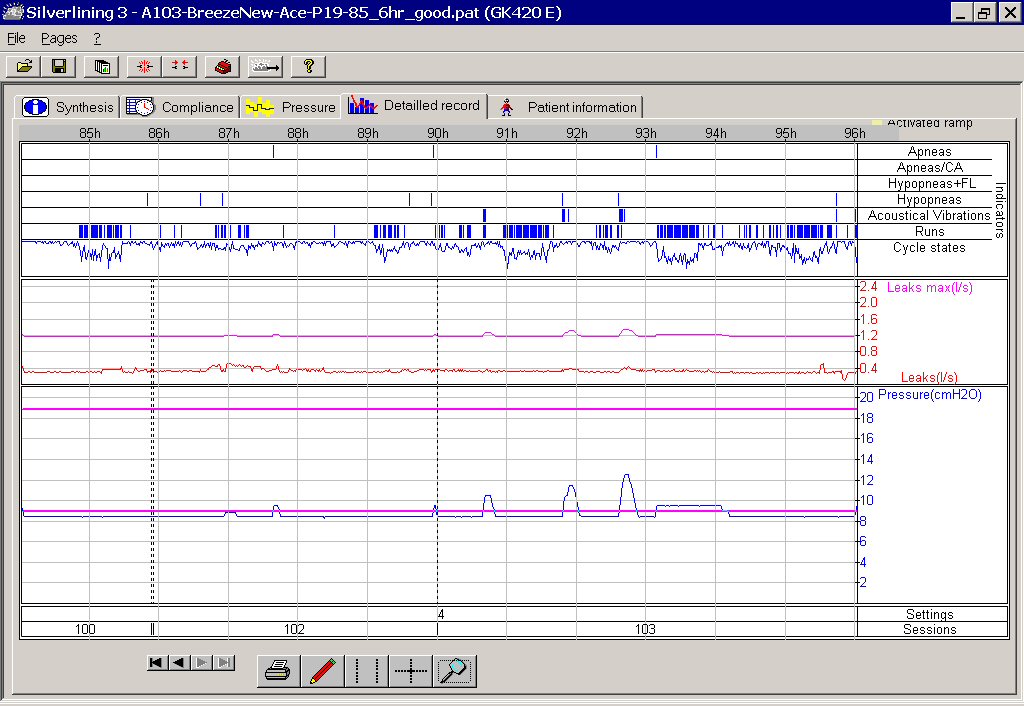
Below are a couple of pictures of the 420E in action, showing how IFL1 being on (it is "On" by default from the mfgr) didn't suit me at all. And how well things settled down after IFL1 was off. This is why, although I personally love the little 420E, it's not the autopap I'd generally recommend for new people.
Not unless they are going to use the software and are aware of what IFL1 might do with some people. And not as long as it comes from the manufacturer with IFL1 turned on. And not as long as the DME setting up a 420E for a new user doesn't know they had better check a download after the very first night or two. And not as long as the DME might not have a clue about what to look for to see if IFL1 being on by default is ok for that person.
Yeah, my personal experience colors my recommendations, too. Here's some of my data with the 420E:
Three sessions (1, 2, 3) with IFL1 left ON, using range of 8 - 17 and then 10.5 - 19:
Three sessions (100,102,103) with IFL1 turned OFF, using a range of 8.5 - 19:
ResMed S9 VPAP Auto (ASV)
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Humidifier: Integrated + Climate Control hose
Mask: Aeiomed Headrest (deconstructed, with homemade straps
3M painters tape over mouth
ALL LINKS by rested gal:
viewtopic.php?t=17435
Yeah I thought that was Wally's reports also, my bad. But in your reports, there is a HUGE improvement in the lower chart.rested gal wrote:If you're referring to the PB420E graph on page 2, I still wish I could'a sneaked in there to flip off IFL1.StillAnotherGuest wrote:The above APAP disaster
Might not have made one bit of difference for Wally. Oh, wait, you said that wasn't Wally??? I could have sworn the peaks looked tall enough to be him!
Below are a couple of pictures of the 420E in action, showing how IFL1 being on (it is "On" by default from the mfgr) didn't suit me at all. And how well things settled down after IFL1 was off. This is why, although I personally love the little 420E, it's not the autopap I'd generally recommend for new people.
Not unless they are going to use the software and are aware of what IFL1 might do with some people. And not as long as it comes from the manufacturer with IFL1 turned on. And not as long as the DME setting up a 420E for a new user doesn't know they had better check a download after the very first night or two. And not as long as the DME might not have a clue about what to look for to see if IFL1 being on by default is ok for that person.
my personal experience colors my recommendations, too. Here's some of my data with the 420E:
Three sessions (1, 2, 3) with IFL1 left ON, using range of 8 - 17 and then 10.5 - 19:
Three sessions (100,102,103) with IFL1 turned OFF, using a range of 8.5 - 19:
Notice in the top chart you went to the Maximum pressure setting of 19cm? In the bottom chart you didn't get over 12.5cm but a few times per night.
I may have to order another one of those 420e's again and give it another try (now that we know what IFL1 actually does). Maybe they are a bit more reliable by now. I'm traveling more now anyway. Still have the download cable and Silverlining software somewhere for the one I had.
Okay I got it now, so the general consensus here IS then:
1. SAG and other PSG's techs are always wrong and we should never rely on them for finding the correct pressure (sorry SAG some beach, by Blake Skelton).
2. We should open our autopaps up from 4cm to 20cm and just let her rip!
3. Chin straps are optional should doing that blow the top of your head off, should that happen the chin strap will hold it on so you don't lose anything.
4. Why is a Digital Rectal Exam called that when it is done with an analog finger in a glove?
-
neversleeps

- Posts: 1141
- Joined: Wed Apr 20, 2005 7:06 pm
- Location: Minnesota
I believe it's called a digital rectal exam because of the one/zero answer invariably returned by this medical procedure.snoredog wrote:Why is a Digital Rectal Exam called that when it is done with an analog finger in a glove?
This Medical Test's Two Answers: "One" or "Zero"
The Prompting Medical Question: "Wow! How many index fingers did your hand end up with after performing a rectal exam on that really uptight patient?"
Digital... right? One/zero.
You must really have some reading comprehension problems.Snoredog wrote:Okay I got it now, so the general consensus here IS then:
1. SAG and other PSG's techs are always wrong and we should never rely on them for finding the correct pressure (sorry SAG some beach, by Blake Skelton).
2. We should open our autopaps up from 4cm to 20cm and just let her rip!
3. Chin straps are optional should doing that blow the top of your head off, should that happen the chin strap will hold it on so you don't lose anything.
4. Why is a Digital Rectal Exam called that when it is done with an analog finger in a glove?
I'm a programmer Jim, not a doctor!
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
I'm Dickens, He's Fenster
You be the straight guy, I'll do the comedy.-SWS wrote:I believe it's called a digital rectal exam because of the one/zero answer invariably returned by this medical procedure.snoredog wrote:Why is a Digital Rectal Exam called that when it is done with an analog finger in a glove?
This Medical Test's Two Answers: "One" or "Zero"
The Prompting Medical Question: "Wow! How many index fingers did your hand end up with after performing a rectal exam on that really uptight patient?"
Digital... right? One/zero.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.
-
StillAnotherGuest
- Posts: 1005
- Joined: Sun Sep 24, 2006 6:43 pm
There's A Reason It Do What It Do
BTW, that APAP gone awry did just swimmingly with the ASV.rested gal wrote:If you're referring to the PB420E graph on page 2, I still wish I could'a sneaked in there to flip off IFL1.StillAnotherGuest wrote:The above APAP disaster
Might not have made one bit of difference for Wally. Oh, wait, you said that wasn't Wally??? I could have sworn the peaks looked tall enough to be him!
I thought Wally started out with the Respironics AutoBiPAP pretty much from Day 1.
Hey, RG, I think those PLMs would stand an equal chance of running your pressures up. That, and your waveform does look a little flat to begin with. By eyeball, I wouldn't have been surprised if the 420 didn't run the pressure up even without IFL1 on.

I mean, at 8 and change, there's still stuff there that needs to be addressed.
SAG
Aromatherapy may help CPAP compliance. Lavender, Mandarin, Chamomile, and Sweet Marjoram aid in relaxation and sleep. Nature's Gift has these and a blend of all four called SleepEase.