





While waiting for my Remstar Auto to arrive from cpap.com (UPS says Friday), I've been thinking about apap operation.
Please correct me if I'm wrong:
1) Pressure level is increased by "events" (apneas etc)
2) In the absence of such "events" the pressure will relax to the minimum.
So the question is: what maintains a constant apap pressure during sleep? It must be a continuing series of events at a frequency that corresponds to the relaxation rate of the machine. According to this argument, an apap machine cannot reduce the AHI to zero. It requires a (small) number of events/hour to keep the pressure at an elevated level.
So apap users should not expect to see an AHI of zero in the reports.
Am I right, or am I right?
derek
Can APAP eliminate apneas?


13 posts
• Page 1 of 1
-
wading thru the muck!

- Posts: 2799
- Joined: Tue Oct 19, 2004 11:42 am
-
Sleeping With The Enemy
- Posts: 454
- Joined: Tue Jan 25, 2005 11:54 pm
- Location: Minnesota
Okay, call me dumb...
I would also like to know about how the straight CPAP works....in reference to this topic.
Thanks for letting me ask dumb questions, sometimes several times on this forum, before it sinks in.
I'm going on no REM sleep, please understand.
Heidi
Thanks for letting me ask dumb questions, sometimes several times on this forum, before it sinks in.
I'm going on no REM sleep, please understand.
Heidi

Re: Okay, call me dumb...
Trust me, Heidi, I totally feel your pain.hhunt wrote:I'm going on no REM sleep, please understand.
Liam, who is a gentleman, and so even on this Mardi Gras evening, her pain is ALL he's trying to feel.
_________________
| Machine | Mask | |
 |  |
Heidi,
If I understand your question, the straight CPAP works by providing a constant pressure at the mask to maintain an "air splint" that keeps the throat open. No smarts at all - just a dumb machine that does what the clinician set it up to do, night after night, after night... until a new titration and a new pressure setting.
I have ordered the "smart" autopap for several reasons:
1) As an engineer, I cannot see that I will need a constant pressure at all times, both in the short term, and the long term. My titrated pressure of 12 cm is a guess based on 3-4 hours of sleep. There was even disagreement between people who read my charts on what I need.
2) Even though I have good respiritory function, and am active, I have found myself waking in the morning feeling short of breath, and sort of sore in the lungs from exhaling against the pressure. My hope is that the APAP will keep the average pressure through the night lower.
3) I am having trouble getting to sleep with the CPAP running. I am presuming that the APAP will keep the pressure at the minimum until I fall asleep (much better than a ramp).
4) I am looking forward to monitoring my nightly antics with the Encore Pro software.
derek
who deep down doesn't think he has OSA. It's all a viscious plot to drive me crazy
If I understand your question, the straight CPAP works by providing a constant pressure at the mask to maintain an "air splint" that keeps the throat open. No smarts at all - just a dumb machine that does what the clinician set it up to do, night after night, after night... until a new titration and a new pressure setting.
I have ordered the "smart" autopap for several reasons:
1) As an engineer, I cannot see that I will need a constant pressure at all times, both in the short term, and the long term. My titrated pressure of 12 cm is a guess based on 3-4 hours of sleep. There was even disagreement between people who read my charts on what I need.
2) Even though I have good respiritory function, and am active, I have found myself waking in the morning feeling short of breath, and sort of sore in the lungs from exhaling against the pressure. My hope is that the APAP will keep the average pressure through the night lower.
3) I am having trouble getting to sleep with the CPAP running. I am presuming that the APAP will keep the pressure at the minimum until I fall asleep (much better than a ramp).
4) I am looking forward to monitoring my nightly antics with the Encore Pro software.
derek
who deep down doesn't think he has OSA. It's all a viscious plot to drive me crazy
APAP
Hi Derek:
Even tho' I'm a hose head going on about 2 wks. and hardly an expert by any stretch of imagination, I wanted the APAP for exactly the reasons that you so aptly put it. During the titration study, having been told little to nothing what to expect ''or'' feel, I woke up with a sinus head worse than a hose head. No humidification. I was able to get it out of the techie that my titrated pressure for the night was 12.5. However, my report, which the dr. called FABULOUS FANTASTIC, I had 19 episodes, I thought on the high side. But in comparison to my diagnostic study 2 wks before, where I had 133 episodes, most hypop's, I guess 19 sounded good to him. How I would've known anything. I was bummed out when I'd glance over at my PB 420E APAP and my setting was low, 4, 5, 6's. But exactly that reason you mention, who wants to feel that you're exhaling against a feeling of intense lung pressure. As an asthmatic I am very aware of the slightest tweak in breathing, pressure, etc. Only a few x's this wk so far, have i noticed a heavier feeling in my chest, but I don't want to ''look at the number'' for fear of waking myself even more. I have a very hard time falling asleep, but I have to say, WHILE KNOCKING ON A THICK PC OF WOOD, that it seems the last few days I've been falling asleep faster, and with less sleep med combo's to knock myself out with.
We are works in progress. I treat ea.night as a night that I am trying to improve my health which isn't the best, and before more complications set in, try to help myself.
The only saying goes, ''if you want something done, do it yourself, " right?
Good Luck, and keep reading, I've learned all I know from this board. Learning and smilin' --------------------this is what I call this msg. board.
Even tho' I'm a hose head going on about 2 wks. and hardly an expert by any stretch of imagination, I wanted the APAP for exactly the reasons that you so aptly put it. During the titration study, having been told little to nothing what to expect ''or'' feel, I woke up with a sinus head worse than a hose head. No humidification. I was able to get it out of the techie that my titrated pressure for the night was 12.5. However, my report, which the dr. called FABULOUS FANTASTIC, I had 19 episodes, I thought on the high side. But in comparison to my diagnostic study 2 wks before, where I had 133 episodes, most hypop's, I guess 19 sounded good to him. How I would've known anything. I was bummed out when I'd glance over at my PB 420E APAP and my setting was low, 4, 5, 6's. But exactly that reason you mention, who wants to feel that you're exhaling against a feeling of intense lung pressure. As an asthmatic I am very aware of the slightest tweak in breathing, pressure, etc. Only a few x's this wk so far, have i noticed a heavier feeling in my chest, but I don't want to ''look at the number'' for fear of waking myself even more. I have a very hard time falling asleep, but I have to say, WHILE KNOCKING ON A THICK PC OF WOOD, that it seems the last few days I've been falling asleep faster, and with less sleep med combo's to knock myself out with.
We are works in progress. I treat ea.night as a night that I am trying to improve my health which isn't the best, and before more complications set in, try to help myself.
The only saying goes, ''if you want something done, do it yourself, " right?
Good Luck, and keep reading, I've learned all I know from this board. Learning and smilin' --------------------this is what I call this msg. board.
derek wrote:Heidi,
If I understand your question, the straight CPAP works by providing a constant pressure at the mask to maintain an "air splint" that keeps the throat open. No smarts at all - just a dumb machine that does what the clinician set it up to do, night after night, after night... until a new titration and a new pressure setting.
I have ordered the "smart" autopap for several reasons:
1) As an engineer, I cannot see that I will need a constant pressure at all times, both in the short term, and the long term. My titrated pressure of 12 cm is a guess based on 3-4 hours of sleep. There was even disagreement between people who read my charts on what I need.
2) Even though I have good respiritory function, and am active, I have found myself waking in the morning feeling short of breath, and sort of sore in the lungs from exhaling against the pressure. My hope is that the APAP will keep the average pressure through the night lower.
3) I am having trouble getting to sleep with the CPAP running. I am presuming that the APAP will keep the pressure at the minimum until I fall asleep (much better than a ramp).
4) I am looking forward to monitoring my nightly antics with the Encore Pro software.
derek
who deep down doesn't think he has OSA. It's all a viscious plot to drive me crazy
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
derek, I shouldn't even attempt these techie type questions, but what you asked was so interesting. I may be way off, but I look at it as whatever low pressure we have set on our autopaps as being what "maintains" apap pressure until something about our air flow characteristics change. A change would be the signal to the autopap that "something was about to happen" and cause the autopap to take action, upping the pressure to prevent a slightly "beginning to collapse" throat from worsening.
I'm probably misunderstanding what you asked, but if you mean do we have to actually have events like apneas/hypopneas throughout the night to make the autopap keep doing its job of keeping the throat open, I don't think that's the case.
As Wader said, if you can keep the AHI below 5, that's considered good. Low AHI, in and of itself, might not really correlate to "feeling better" all the time. Better bottom line is how we feel. But generally it's a good indication of how treatment is going if the AHI is lower rather than higher.
I've seen my AHI be 0.0 perhaps three times in the past 5 months. Each of those times was during a nap of one or not more than two hours...never throughout an entire night. I've also seen my AHI be 1.whatever, after a one hour nap, so it can certainly vary. Usually my AHI is 1.something or 2.something during a 6 or 7 hour night.
I don't think there's any particular benefit in having a 0.0 AHI compared to an AHI that did record a few things.
I should mention I use a pressure range where I've set my "low" higher than most people have theirs. I've set my autopap for a range of 10-16. I like the low up at 10 because if I lie there with machine going at, say 8, and try to totally relax my throat (simulating the relaxation of sleep) I can feel some throat closure and would produce a snore. 10 keeps it open completely, and my machine uses 10 or 11 most of the night, occasionally hitting 13 briefly.
One might say I'm, in effect, using my autopap as a straight cpap of 10 or 11, but with the benefit of "autopap" in setting a higher ceiling to allow for catching occasional events that might need more pressure. Of course, the C-Flex of my Remstar Auto with C-flex allows me to have that low set up pretty high and enjoy considerably less pressure on each exhalation. Quite comfortable for me.
I'm probably misunderstanding what you asked, but if you mean do we have to actually have events like apneas/hypopneas throughout the night to make the autopap keep doing its job of keeping the throat open, I don't think that's the case.
As Wader said, if you can keep the AHI below 5, that's considered good. Low AHI, in and of itself, might not really correlate to "feeling better" all the time. Better bottom line is how we feel. But generally it's a good indication of how treatment is going if the AHI is lower rather than higher.
I've seen my AHI be 0.0 perhaps three times in the past 5 months. Each of those times was during a nap of one or not more than two hours...never throughout an entire night. I've also seen my AHI be 1.whatever, after a one hour nap, so it can certainly vary. Usually my AHI is 1.something or 2.something during a 6 or 7 hour night.
I don't think there's any particular benefit in having a 0.0 AHI compared to an AHI that did record a few things.
I should mention I use a pressure range where I've set my "low" higher than most people have theirs. I've set my autopap for a range of 10-16. I like the low up at 10 because if I lie there with machine going at, say 8, and try to totally relax my throat (simulating the relaxation of sleep) I can feel some throat closure and would produce a snore. 10 keeps it open completely, and my machine uses 10 or 11 most of the night, occasionally hitting 13 briefly.
One might say I'm, in effect, using my autopap as a straight cpap of 10 or 11, but with the benefit of "autopap" in setting a higher ceiling to allow for catching occasional events that might need more pressure. Of course, the C-Flex of my Remstar Auto with C-flex allows me to have that low set up pretty high and enjoy considerably less pressure on each exhalation. Quite comfortable for me.
Rested,
If you register an AHI of 0 it means that you had no events during the session, therefore the APAP would sit at the minimum pressure the whole time, which is consistent with my original conjecture.
This is slightly different from saying that APAP eliminated all events that session - you were lucky on those occasions and there was nothing broken to fix May you have many more like that!
derek
If you register an AHI of 0 it means that you had no events during the session, therefore the APAP would sit at the minimum pressure the whole time, which is consistent with my original conjecture.
This is slightly different from saying that APAP eliminated all events that session - you were lucky on those occasions and there was nothing broken to fix May you have many more like that!
derek
Precursors
No, Rested Gal got it right. You can register an AHI of 0.0 and have prevented apneas by proactively elevating pressure before any apneas or hypopneas occurred. Recall that, exactly as rested Gal said, the AutoPAP will look for highly predictive precursors to trigger on. Those precursors can be snore, flow limitations, or even sequential lesser flow limited respiratory cycles (called "intermediate" cycles).
An AHI of 0.0 can happen because they were all addressed at the minimum pressure as well, as Derek stated. That would be an AHI of 0.0 happening via two different scenarios. The third scenario is the least likely for true apneics: there were no apneas/hypopneas that night to address at any pressure.
An AHI of 0.0 can happen because they were all addressed at the minimum pressure as well, as Derek stated. That would be an AHI of 0.0 happening via two different scenarios. The third scenario is the least likely for true apneics: there were no apneas/hypopneas that night to address at any pressure.
Of course,,,
-SWS is correct. I was thinking of purely reactive APAP. Proactive algorithms can act to prevent events that would have happened without an APAP pressure bump and thus keep the AHI at zero,
Silly me...
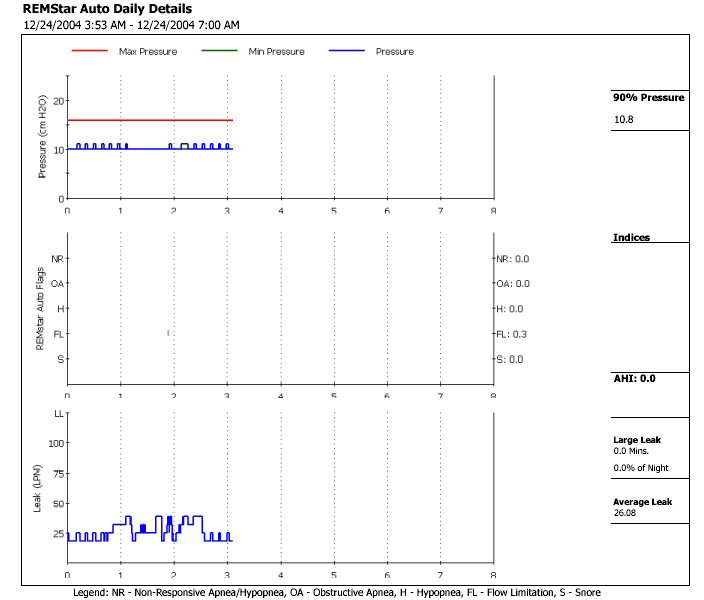
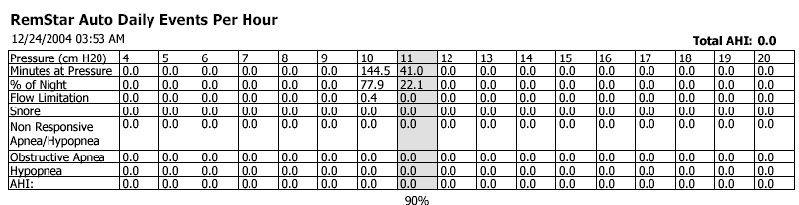
Thanks for the charts Rested Gal, I look forward to being able to look at my own response
derek
who woke at 3am with a blocked nose
Silly me...
Thanks for the charts Rested Gal, I look forward to being able to look at my own response
derek
who woke at 3am with a blocked nose
Reactive
That was quite impressive for someone who hasn't even laid their hands on an AutoPAP yet, Derek. What you described also happens with an AutoPAP---and exactly the way you described it.
That impresses me immensely! As Rested Gal would say: "You're a good 'un!"
-SWS
That impresses me immensely! As Rested Gal would say: "You're a good 'un!"
-SWS
Shortness of Breath
Derek, that sounds like the same dyspnea I was experiencing on CPAP at only 10 cm. I experience it much less on AutoPAP. My primary physician speculated that my alveoli were actually overinflating and stretching a bit, leaving me with slight "COPD-like" dyspnea. In one way, shape, or form the body has to somehow resolve that fixed pressure when it's not being used to correct an apnea...derek wrote: Even though I have good respiritory function, and am active, I have found myself waking in the morning feeling short of breath, and sort of sore in the lungs from exhaling against the pressure.
13 posts
• Page 1 of 1