I would be looking for these in Sleepyhead:dudemandude wrote:Hey Tan could you elaborate on what things you looked at in Sleepyhead to get an understanding of what you could improve in your treatment? I've spent a lot of time lurking these forums learning to understand what I'm looking at and have attempted to find clues as to what I could do by looking at my Sleepyhead results at various pressures to no avail. While my sleep hygiene right now is not very good, I did fix it at various points in my ordeal without any real significant improvements unfortunately. Also how did you eventually settle down on the VPAP solution? Did you ask your doctor to titrate you on it after CPAP failed? Thanks so much for your advice, UARS has proven to be a lot harder to deal with then I had hoped.tan wrote:I had a very similar story with UARS: low AHI, high RDI, honeymoon with APAP, then a "divorce" from it, looking for solutions, including sleep dentist, one count of attempted surgery (changed my mind), but finally found a solution with VPAP and remain "married" to it happily ever every since.
UARS patients natural have a light sleep. Practicing a good sleep hygiene is a good start. Then, you use Sleepy Head to investigate what else may be causing sleep distrubances
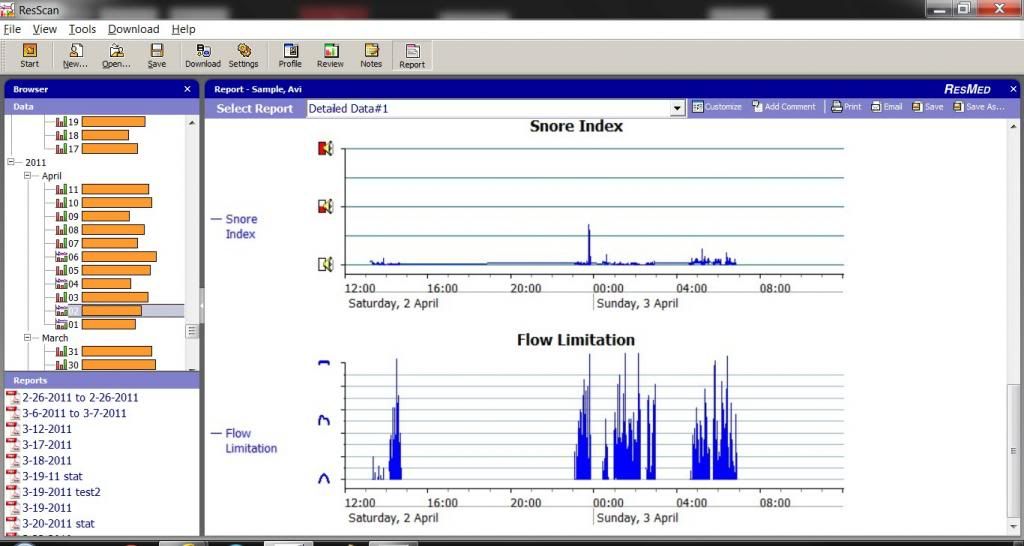
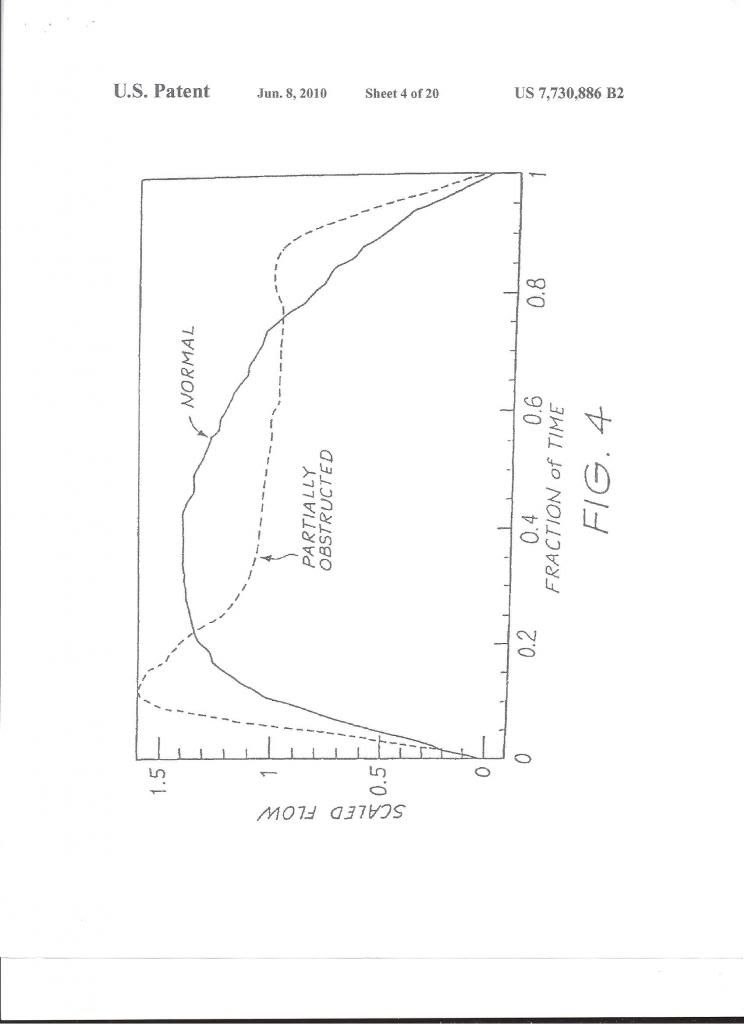
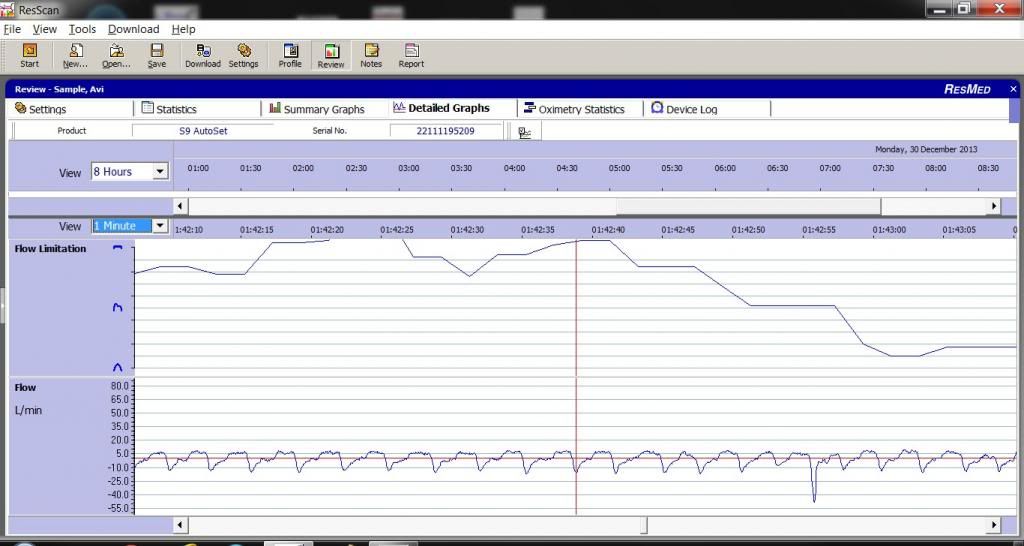
1waveform, manually, breath by breath, ideally it should be a regular pattern. RERAs make it irregular - to have an idea whether you have UARS
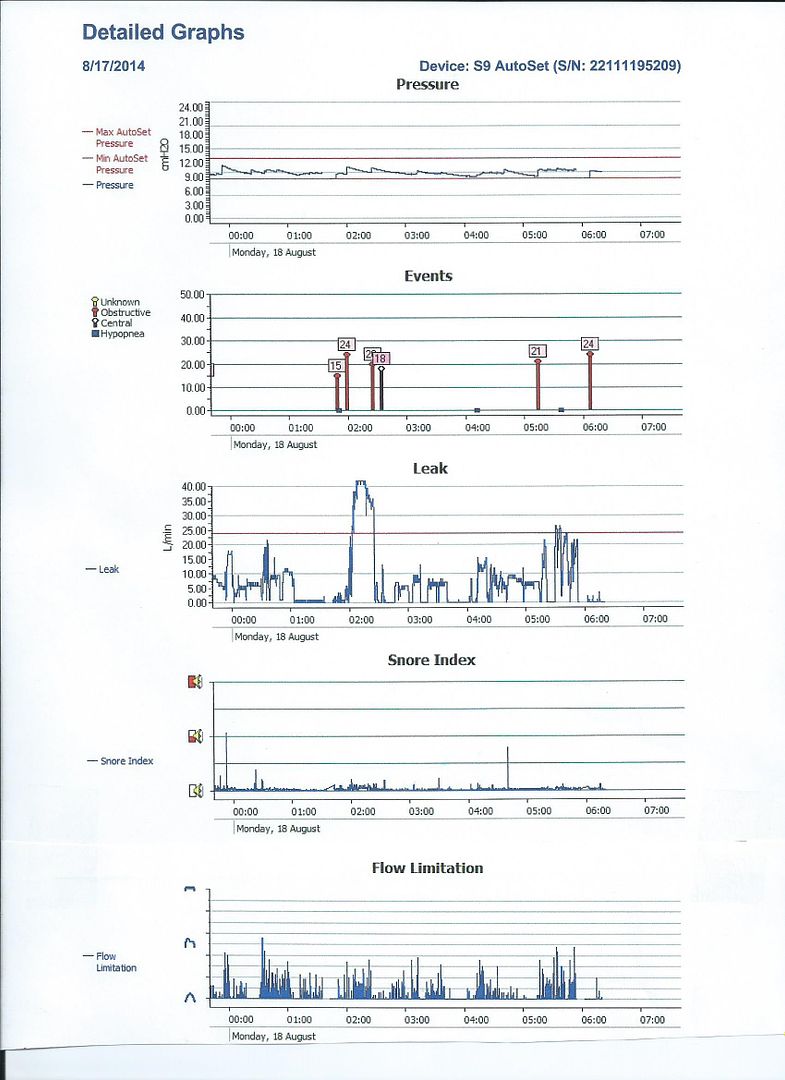
2) flow limitations
3) leaks
Of course, titration is best done in the lab, but good luck having sleep study approved for UARS. My insurance told me to fuck off. On the other hand, titration at home offers familiar environment but it in case of UARS it involves a great deal of trial and error since AHI ain't mean shit and RDI cannot be properly measured.
I resorted to VPAP because I had been influenced by Krakow's articles... Not that they had been particularly helpful. I had been blindly increasing pressures with APAP and felt difficulties on exhale and APAP cannot have EPR over 3. So I decided to waste cash of VPAP from a craigslist ad ($800). I experimented some more: VPAP has trigger/cycle sensitivity configurable (my personal settings are very high, which I found most comfortable) and also settled and 9 exhale, 13 inhale, pressure support 4 and I also tape my mouth and use full face mask and use nasal strips to expand my flimsy nostrils. A lot of variables, as you can see. Not necessarily applicable to your case.
Needless to say, stress, bad sleep hygiene could still my ruin my sleep.