






How about episode 96, and isn't it obviously a RERA?Morbius wrote:Yeah, I'm really not seeing that there. Looks more like sleep stage instability (given the time) with some CAP stuff:musculus wrote:Chest and abdomen movements suggest the arousals are RERAs
http://www.aastweb.org/resources/a2zzz/ ... khardt.pdf
Flow limitation: when are they considered significant?
Re: Flow limitation: when are they considered significant?

Re: Flow limitation: when are they considered significant?
Since we're looking at the NPSG, we can appropriately identify the RERA, which is technically the arousal. With that in mind, which arousal are you calling a RERA? In the first one, although there is some FL it continues for at least one and perhaps 2 breaths. Recovery breaths do not start until ~5 seconds after the arousal, and they are not particularly impressive. Increased effort is accompanied by increased flow, so that is normal (middlie of Epoch 96). Thus, I would call that a spontaneous arousal. That whole area looks to be sleep instability. Given those eye movements, I'd be hard-pressed to call anything in there N2.musculus wrote:How about episode 96, and isn't it obviously a RERA?Morbius wrote:Yeah, I'm really not seeing that there. Looks more like sleep stage instability (given the time) with some CAP stuff:musculus wrote:Chest and abdomen movements suggest the arousals are RERAs
http://www.aastweb.org/resources/a2zzz/ ... khardt.pdf
The second arousal cannot be a RERA because there is no FL.

Re: Flow limitation: when are they considered significant?
Jumping in from another thread. I have a low average AHI (.5) and a consistently ragged flow limitation line. The last few nights I've tried EPR 3 to see if it affects my FL and sleep quality, and it totally does. I've experienced a dramatic improvement in restfulness, aerophagia, and leaks. It's not entirely clear that FL was the culprit, but the EPR is helping, however it's doing it. I've been struggling for two years so it's nice to take a measurable step in the right direction.
All else being equal, does a BiLevel machine handle inhale/exhale pressure changes more comfortably than an APAP with EPR? For example, would IPAP 9cm and EPAP 6cm on a BiLevel feel the same as an Auto providing 9cm with an EPR of 3? Or does it manage the changes more smoothly?
All else being equal, does a BiLevel machine handle inhale/exhale pressure changes more comfortably than an APAP with EPR? For example, would IPAP 9cm and EPAP 6cm on a BiLevel feel the same as an Auto providing 9cm with an EPR of 3? Or does it manage the changes more smoothly?
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
Re: Flow limitation: when are they considered significant?
I vaguely remember a few people here swear that Auto with ERP==3 and BiLevel with PS==3 are quite different things!SteveGold wrote:Jumping in from another thread. I have a low average AHI (.5) and a consistently ragged flow limitation line. The last few nights I've tried EPR 3 to see if it affects my FL and sleep quality, and it totally does. I've experienced a dramatic improvement in restfulness, aerophagia, and leaks. It's not entirely clear that FL was the culprit, but the EPR is helping, however it's doing it. I've been struggling for two years so it's nice to take a measurable step in the right direction.
All else being equal, does a BiLevel machine handle inhale/exhale pressure changes more comfortably than an APAP with EPR? For example, would IPAP 9cm and EPAP 6cm on a BiLevel feel the same as an Auto providing 9cm with an EPR of 3? Or does it manage the changes more smoothly?
Speaking from my experience, in order to make my Bilevel work for me, I had to make its trigger/cycle very sensitive. With default settings, which were medium, it was harder for me to tolerate
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |

Re: Flow limitation: when are they considered significant?
I believe you're mistaken on that account.tan wrote:I vaguely remember a few people here swear that Auto with ERP==3 and BiLevel with PS==3 are quite different things!SteveGold wrote:All else being equal, does a BiLevel machine handle inhale/exhale pressure changes more comfortably than an APAP with EPR? For example, would IPAP 9cm and EPAP 6cm on a BiLevel feel the same as an Auto providing 9cm with an EPR of 3? Or does it manage the changes more smoothly?
it all depends on which bilevel you're talking about though, staying in the resmed world, epr3 on a cpap/autoset and a ps of 3 on a vpap in s mode with easybreath on creates very similar pressure changes.
turn off easybreath and the transitions are much more binary, though it's adjustable with the risetime setting. cranking rise time way up gives a similarish curve, but still not quite the same.
vauto mode has easybreath on in it's pressure control, giving a smooth rise akin to the epr.
Last edited by palerider on Fri Nov 16, 2018 8:26 pm, edited 1 time in total.
Get OSCAR
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
-
Greg Riddle
- Posts: 409
- Joined: Wed Aug 13, 2014 4:48 pm
- Contact:
Re: Flow limitation: when are they considered significant?
The resmed vpap with a ps of 3 id's similar to the auto with epr if 3.tan wrote:I vaguely remember a few people here swear that Auto with ERP==3 and BiLevel with PS==3 are quite different things!SteveGold wrote:Jumping in from another thread. I have a low average AHI (.5) and a consistently ragged flow limitation line. The last few nights I've tried EPR 3 to see if it affects my FL and sleep quality, and it totally does. I've experienced a dramatic improvement in restfulness, aerophagia, and leaks. It's not entirely clear that FL was the culprit, but the EPR is helping, however it's doing it. I've been struggling for two years so it's nice to take a measurable step in the right direction.
All else being equal, does a BiLevel machine handle inhale/exhale pressure changes more comfortably than an APAP with EPR? For example, would IPAP 9cm and EPAP 6cm on a BiLevel feel the same as an Auto providing 9cm with an EPR of 3? Or does it manage the changes more smoothly?
Speaking from my experience, in order to make my Bilevel work for me, I had to make its trigger/cycle very sensitive. With default settings, which were medium, it was harder for me to tolerate
I have done a lot of experimenting in the last 2 1/2 months. The one thing that has reduced flow limitations want epap it was pressure support. I have found that any ps below 7.2 causes short apnea events very frequently whi tin the first hour of try to sleep. I find it very hard to get any restful sleep. The odd thing is the higher the epap it's the worse the apnea event was. The last experiment was I kept epap at 25 and adjusted the epap from 16.4 to 20 in increments of .2. The closer I got to 20 epap and 5ps the worse the event got
Flow limitations decrease to extremely low levels for me with the ps above 8.5
_________________
| Machine: AirCurve™ 10 VAuto BiLevel Machine with HumidAir™ Heated Humidifier |
| Mask: Quattro™ FX Full Face CPAP Mask with Headgear |
-
donewithbeingtired

- Posts: 34
- Joined: Thu Feb 05, 2015 4:04 pm
Re: Flow limitation: when are they considered significant?
i am jumping in too with a similar question on this...i am not as familiar with all the machine specific jargon.
i have low AHI <1.0 using CPAP mode, but crappy results (tired, foggy, etc.) but have recently been using it in APAP mode with the two pressures set equally at 9.5cm just so I can get a look at the FL info.
this came from following this thread.
i only get 1 or 2 events over the course of a night's sleep, but then regular 20-30 min FLs all night.
i have the "Aflex setting at 3"...its this the corollary to EPR? trying to limit the FLs as an experiment to get better results.
thx, T
i have low AHI <1.0 using CPAP mode, but crappy results (tired, foggy, etc.) but have recently been using it in APAP mode with the two pressures set equally at 9.5cm just so I can get a look at the FL info.
this came from following this thread.
i only get 1 or 2 events over the course of a night's sleep, but then regular 20-30 min FLs all night.
i have the "Aflex setting at 3"...its this the corollary to EPR? trying to limit the FLs as an experiment to get better results.
thx, T
_________________
| Machine: PR System One REMStar 60 Series Auto CPAP Machine |
| Mask: Quattro™ FX Full Face CPAP Mask with Headgear |
Sleepyhead
Re: Flow limitation: when are they considered significant?
*flex and epr are different, they both offer some relief of the pressure, but in different ways.donewithbeingtired wrote:i have the "Aflex setting at 3"...its this the corollary to EPR? trying to limit the FLs as an experiment to get better results.
Get OSCAR
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
-
donewithbeingtired
- Posts: 34
- Joined: Thu Feb 05, 2015 4:04 pm
Re: Flow limitation: when are they considered significant?
I see on my machine there is "Aflex" and also something called "System One Resistance".*flex and epr are different, they both offer some relief of the pressure, but in different ways.
If I am trying to optimize and address these FLs and get beyond this low AHI number, then should I be focusing on one of these versus the other?
Can I get a pointer to how you use them?
Thx.
_________________
| Machine: PR System One REMStar 60 Series Auto CPAP Machine |
| Mask: Quattro™ FX Full Face CPAP Mask with Headgear |
Sleepyhead

Re: Flow limitation: when are they considered significant?
I doubt that AFlex or the Resistance control will impact the FLs but you can play with them to see if it does or if it generally feels better.donewithbeingtired wrote: I see on my machine there is "Aflex" and also something called "System One Resistance".
If I am trying to optimize and address these FLs and get beyond this low AHI number, then should I be focusing on one of these versus the other?
Can I get a pointer to how you use them?
AFlex is nothing more than exhale relief...will give up to 2 cm relief (at the setting of 3) depending on how forceful you breathe.
http://aflex.respironics.com/
It may or may not impact the FLs because there are so many variables in how people breathe so I usually tell people to use the setting that feels more natural to them...be it off, 1, 2 or 3. Play with it to see what is the most comfortable for you.
http://aflex.respironics.com/
Resistance control has to do with the innate resistance in the masks and it varies a lot between masks and sizes and Respironics only offers the setting that should be used with Respironics masks.
See these 2 links
http://www.healthcare.philips.com/main/ ... ontrol.wpd
viewtopic/t86975/Explain-Mask-Resistance-Setting.html
If you are using a Respironics mask the Resistance control setting should be on the packaging somewhere.
To be honest...I played with Resistance control settings from Off (that's what is suggested to use for non Respironics masks) to the highest and I couldn't really tell any difference at all in how it felt or in my therapy but it's something that people can try to see if it helps anything or not.
_________________
| Machine: AirCurve™ 10 VAuto BiLevel Machine with HumidAir™ Heated Humidifier |
| Additional Comments: Mask Bleep Eclipse https://bleepsleep.com/the-eclipse/ |
I may have to RISE but I refuse to SHINE.
-
Guest1
Re: Flow limitation: when are they considered significant?
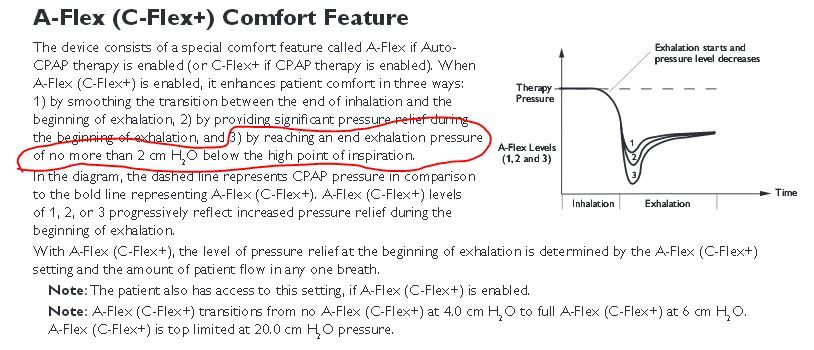
All A-Flex levels ultimately give a pressure relief of 2cm h20. So if your IPAP is 10cm, your EPAP will be 8cm. When exhalation starts, the pressure dips a bit further than 2cm (depending on aflex setting of 1,2,3) but ultimately rests on 2cm relief. There is a graph on aflex DOT respironics DOT com that explains it.donewithbeingtired wrote:I see on my machine there is "Aflex" and also something called "System One Resistance".*flex and epr are different, they both offer some relief of the pressure, but in different ways.
If I am trying to optimize and address these FLs and get beyond this low AHI number, then should I be focusing on one of these versus the other?
Can I get a pointer to how you use them?
Thx.
EPR actually gives 3 levels of pressure relief 1cm, 2cm and 3cm h20 on settings of 1,2,3 respectively.
The resistance control function makes sure that the pressure delivered by the system is the actual pressure in the mask although it doesn't differ by much. If you are using a non-respironics mask, just set the system one resistance settings to the respironics mask which is similar to yours. For example, I use a resmed P10 large pillows. From respironics literature, I gathered that X1 setting will work for this mask. I use X1.
Re: Flow limitation: when are they considered significant?
Actually AFlex (CFlex +) actual amount of exhale relief is flow based so the stronger the breathing the greater the reduction UP TO 2 cm at the highest setting which is 3 and less than that for lesser settings.
And it isn't active unless the minimum pressure setting is at least 6 cm.
And it isn't active unless the minimum pressure setting is at least 6 cm.

_________________
| Machine: AirCurve™ 10 VAuto BiLevel Machine with HumidAir™ Heated Humidifier |
| Additional Comments: Mask Bleep Eclipse https://bleepsleep.com/the-eclipse/ |
I may have to RISE but I refuse to SHINE.
Re: Flow limitation: when are they considered significant?
The second one is RERA. Beginning at the green line, no inflow (FL), then arousal almost at the same time, followed with larger abdomen movement, then inflow resumed.Morbius wrote:Since we're looking at the NPSG, we can appropriately identify the RERA, which is technically the arousal. With that in mind, which arousal are you calling a RERA? In the first one, although there is some FL it continues for at least one and perhaps 2 breaths. Recovery breaths do not start until ~5 seconds after the arousal, and they are not particularly impressive. Increased effort is accompanied by increased flow, so that is normal (middlie of Epoch 96). Thus, I would call that a spontaneous arousal. That whole area looks to be sleep instability. Given those eye movements, I'd be hard-pressed to call anything in there N2.musculus wrote:How about episode 96, and isn't it obviously a RERA?Morbius wrote:Yeah, I'm really not seeing that there. Looks more like sleep stage instability (given the time) with some CAP stuff:musculus wrote:Chest and abdomen movements suggest the arousals are RERAs
http://www.aastweb.org/resources/a2zzz/ ... khardt.pdf
The second arousal cannot be a RERA because there is no FL.