(I would call you "Sleepy" but don't want to imply you are one of the Seven Dwarfs--and that would be six letters anyway.)

Yes, this is scary, particularly for someone who had a long and difficult adjustment period:Sludge wrote:Even more important are the criteria for which they snatch the machine back:robysue wrote:Medicare is up front about exactly when they will and will not pay for a CPAP trial.
http://www.cms.gov/Outreach-and-Educati ... 905064.pdf
So if you crash and burn for the first 3-4 months in terms of daytime functioning because you're having a real tough time learning how to sleep with a six foot hose attached to your nose and a machine blowing air down your throat all night, it looks like Medicare can decide to discontinue paying for the PAP even if you are compliant and working hard on making this crazy therapy work and the compliance data looks good.DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services wrote:
Continuous and Bi-level Positive Airway Pressure
(CPAP/BPAP) Devices:
Complying with Documentation & Coverage Requirements
...
Common PAP Device Errors
...
5. No documentation of the treating physician’s face-to-face re-evaluation, within the first
three months of initiating therapy (but after the 31st day), which documents both improvement
in subjective symptoms of OSA and objective data related to adherence to PAP therapy.
(Emphasis added.)
...
What Do I Need to Know to Prevent Errors?
...
4. Remind the patient that a re-evaluation is required for continuing PAP coverage beyond
the initial 3 months. This re-evaluation must document that the patient is benefiting
from, and adhering to, the PAP therapy as ordered (that is, continued need and
continued use). This requirement may be facilitated by the use of compliance cards/memory
cards in the PAP device. (Emphasis Added)
| Machine: DreamStation BiPAP® Auto Machine |
| Mask: Swift™ FX Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: PR System DreamStation and Humidifier. Max IPAP = 9, Min EPAP=4, Rise time setting = 3, minPS = 3, maxPS=5 |
And this is just plain sad as well as being all too true.Sludge wrote: But the "standard approach" is rapidly becoming do an HST, then here's a 4/20 APAP and GFL.
| Machine: DreamStation BiPAP® Auto Machine |
| Mask: Swift™ FX Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: PR System DreamStation and Humidifier. Max IPAP = 9, Min EPAP=4, Rise time setting = 3, minPS = 3, maxPS=5 |
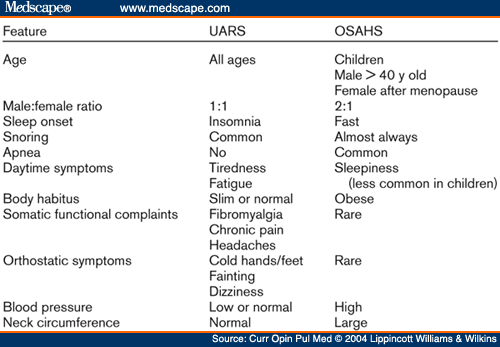
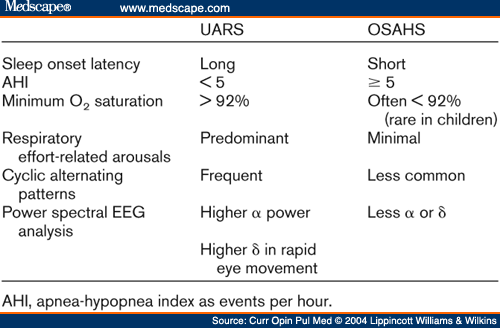
Once again I'm surprised at how close I match the descriptors for UARS and how few of the descriptors for OSAHS "fit me." (Of course by know I also know I should not be surprised at this anymore.)Sludge wrote:Anyway...
| Machine: DreamStation BiPAP® Auto Machine |
| Mask: Swift™ FX Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: PR System DreamStation and Humidifier. Max IPAP = 9, Min EPAP=4, Rise time setting = 3, minPS = 3, maxPS=5 |
Although I can't imply an attorney-client relationship, I still recommend Sludge assert fifth-amendment privilege.. . . just how fuzzy . . . if it's known the insurance company will pay for treating OSA, but will not pay for treating UARS?
robysue wrote: Once again I'm surprised at how close I match the descriptors for UARS and how few of the descriptors for OSAHS "fit me." (Of course by know I also know I should not be surprised at this anymore.)
Sludge, just how fuzzy is the line for scoring Rule 4B "Hypopneas with arousal" vs. RERAs when there's no esophageal pressure transducer used? Particularly if it's known the insurance company will pay for treating OSA, but will not pay for treating UARS?

Setj wrote:robysue wrote: Once again I'm surprised at how close I match the descriptors for UARS and how few of the descriptors for OSAHS "fit me." (Of course by know I also know I should not be surprised at this anymore.)
Sludge, just how fuzzy is the line for scoring Rule 4B "Hypopneas with arousal" vs. RERAs when there's no esophageal pressure transducer used? Particularly if it's known the insurance company will pay for treating OSA, but will not pay for treating UARS?
Do home tests (HST) detect UARS in a patient that does not have apnea or hypopnea?
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Complex Sleep Apnea, mainly CSA, with UARS. RDI of 30 w/o xPAP. |
When I had a HST as a clueless newcomer to the apnea world, I was told that my test could detect UARS. I now realize how impossible that would have been and am shaking my head at what I was led to believe.justinjustin wrote:Setj wrote:robysue wrote: Once again I'm surprised at how close I match the descriptors for UARS and how few of the descriptors for OSAHS "fit me." (Of course by know I also know I should not be surprised at this anymore.)
Sludge, just how fuzzy is the line for scoring Rule 4B "Hypopneas with arousal" vs. RERAs when there's no esophageal pressure transducer used? Particularly if it's known the insurance company will pay for treating OSA, but will not pay for treating UARS?
Do home tests (HST) detect UARS in a patient that does not have apnea or hypopnea?
Almost definitely not. It may be possible to detect some flow limitation that suggest UARS, but without a Pes and/or EEG measuring concomitant arousals, HST cannot reliably detect and confirm UARS.
| Mask: SleepWeaver Elan™ Soft Cloth Nasal CPAP Mask - Starter Kit |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Use SleepyHead |
jnk wrote:I believe that much of Dr. K's genius isn't so much in what he prescribes or how he diagnoses conditions but in how he finds a way to make insurance pay for what he prescribes.
I also believe he and his "people" have a knack for informing some patients about, and getting them excited about, SDB in general and his team's crafted customized approach for those with multiple sleep complications, medical and otherwise, who have failed badly with more standard approaches.
Do I think that sort of thing is necessary for every OSA patient? No. Do I believe he sometimes stumbles onto ways of being extremely helpful to individual patients with nonstandard sleep problems or PAP-therapy complications? Yes.
5K IS a serious hunk of dough,--but hey, if it turns a life around . . .
Just me.
As for UARS, the only reason a lab would have to look for it is if the patient's payers consider that a valid diagnosis for qualifying to try PAP. Otherwise, why look for a condition that will earn the patient the same rights to try a CPAP as a diagnosis of "heebie-jeebies" would? Payers dictate what conditions are looked for, since payers have more control over treatments than doctors do, in this day and age. In my opinion. And I still don't think all payers are on board with the UARS thing, whether docs are or not.
| Mask: Mirage™ FX Nasal CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
I hereby invoke my Fifth Amendment right, and insist upon a fair and speedy public trial by jury.jnk wrote:Although I can't imply an attorney-client relationship, I still recommend Sludge assert fifth-amendment privilege.. . . just how fuzzy . . . if it's known the insurance company will pay for treating OSA, but will not pay for treating UARS?
But preferably, as a general rule, not in that order, as in:Physician wrote: . . . requires a prescription, progress notes, and an abnormal PSG.
Sludge, earlier in this thread, wrote: . . . now got her AHI all the way down to 12.1 from 0.0, . . .
In my opinion, response to therapy is the ultimate diagnostic tool in many instances in which the treatment is harmless to virtually all and is much less costly than the lab work. Why order a CT to see if the aspirin is reducing inflammation? I'll settle for the subjective report from the user instead.Physician wrote:. . . she feels the best she has in a year. . . .
I'll say.jnk wrote:I mean, it's not like there is a big problem with recreational use of PAP therapy out there...
But "IMHO", an unfounded, anonymous, illogical, anectdotal, syllogistic analysis could just as easily be (more, actually) a cover for some nefarious plot (usually involving money).jnk wrote:Then again, personally, I care more about subjective results than squigglies. And:Sludge, earlier in this thread, wrote: . . . now got her AHI all the way down to 12.1 from 0.0, . . .
In my opinion, response to therapy is the ultimate diagnostic tool.Physician wrote:. . . she feels the best she has in a year. . . .
| Mask: Mirage™ FX Nasal CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |