red1,
First the "easy" stuff: To get the image to show up directly in the post, you need to put the link inside an
[ img ] ... [ /img ] command where there are no blanks between the []'s and the img and \img "words". If you Quote this message you'll see how I did it for the links you provided.
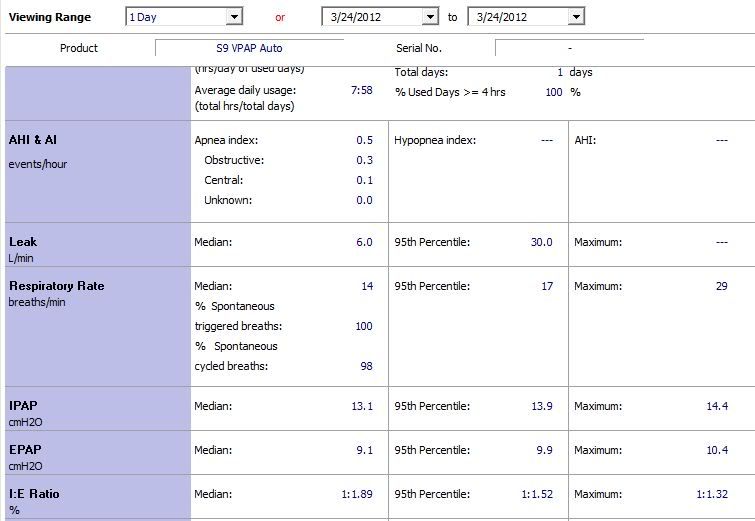
So here are red1's graphs:


Now for the harder stuff.
You write:
Over the last year, my centrals have been kept at about .05. Over the past few months, I began to get the odd day, maybe twice a month, where I would have between a central index of 3 & 6.
Lately, meaning the 8 days, they have been getting higher. Yesterday I had a central index of 11.5 & today, I had a central index of 24.9.
It is really beginning to scare me. I spoke to my sleep doc & respirologist about this a copule months back, she said its nothing & you certainly do not need a vpap adapt sv. Thats when she gave me the Vpap Auto.
.....
Yesterday, the 11.5 was the highest central index I had, but now, the 24.9, wow, thats more then double. I really am at a loss here. I do not know what do do or what to think.
Sounds like a couple of months back you were seeing the odd day here and there with a CAI between 3 and 6. And the sleep doc was probably right at the time: It's nothing to get too worried about if you see one index slightly elevated now and then. Particularly if you can tie the bad numbers to a bad night for sleep in some other sense.
But---something's changed and now you're seeing
very high numbers on a frequent basis. I'd call the sleep doc back on Monday and give a report of the last 7 or 8 days of numbers along with a short synopsis of how you're feeling during the day. Exhausted? Fog brained? OK, but not great? Same as always? Whatever it is, the description of how you're feeling is important for the doc to be able to evaluate the high CAI in context.
During these centrals, the vpap auto pressure does not change at all. I wore my oxymeter last night, the flow of the oxygen levels on the oxymeter report looked just like the respiration rate flow of the ResScan report, where I had the events.
The machine is intentionally designed to NOT change the pressure in response to clear airway events. The rationale: Clear airway events occur with a
unobstructed, non-collapsed airway and are presumed to be central apneas---i.e. the problem is presumed to be caused by the brain failing to send the signal to breath instead of the airway collapsing. Since the airway is already open, there's no physical reason to increase the air pressure (increased air pressure is supposed to make it more difficult for the airway to collapse.) And since some people are prone to develop central apneas at higher pressures, it makes sense to record the CAs, but not respond to them by increasing the pressure since increased pressure may make the situation worse, not better.
I wish I knew what what causing them. Someone mentioned to me a couple months back that the waveform looked like cheyne stokes. I do not have any heart condition that I am aware of. I just went through a stress test, a 48 hour halter monitor, and a echocardiogram & it was all fine. I have a little swelling in my right lower leg, just above the anckle. They did a altrasound & took blood pressures from my legs & it was fine. I do know I my c02 blood work sits at the high end of normal.
How long has the CO2 blood work been at the high end of normal? That could be evidence pointing towards a problem with your body's system to regulate CO2 and that could make it more difficult for your body's automatic nervous system to use CO2 blood levels to trigger breathing in the normal way for sleep breathing. Is the sleep doc aware that you've been tested for heart disease? Is the sleep doc aware of your CO2 blood work? One sad thing about our medical system here in the US is that specialists seldom actually talk to each other. And it's not even clear that specialist A reads what specialist B has written---if specialist B even sends specialist A a copy of the report.
And for what it's worth, to this patient's eyeballs, yes, your breathing pattern does seem to resemble periodic breathing and possibly Cheyne Stokes.
My Spntaneous cycled breathing was way down to 95%. My I & E median ratio was up to 1:2.04 from my average median of 1:1.64
I'm not sure what you are talking about here. I didn't think the S9 VPAP Auto had a mode where it measured spontaneous (patient-triggered/initiated) breaths vs. non-spontaneous (machine-triggered?) breaths since the VPAP Auto is just an Auto Bi-level that does not have the ability to trigger a patient to breathe---i.e. the VPAP Auto does not act like a non-invasive ventilator as near as I know.
Or do you have a VPAP Auto
ST machine set with a back-up breaths per minute rate? That's a different machine altogether and much closer to the VPAP Adapt SV machine.