







Hello there Justbreathe, I saw the post with your graphs and found it extremely strange that you exhibited an enormous amount of Centrals, two hypopneas, and not a single Obstructive apnea. Am curious what your latest graphs look like after the adjustments with your machine. While it may be true that a high pressure setting may be causing this, considering that your machine was set at 9 cmH20, coupled with S9's EPR, it is very unlikely. I'd almost suspect that your machine may not be working properly or at least might be misdiagnosing you. I read along the blog a suggestion for you to take the machine to your DME for examination as well. Maybe you should look into that, too.
As regards MD's, I agree that the best doctors are not necessarily the most educated ones with most letters after their names, but rather the ones that give you the best attention and concern. As such, try to exhaust all avenues first with the pulmonologist before consulting a neurologist.
Good luck on the ASV titration. I hope this resolves your issues. Keep us posted.
Regards,
Tsubs
Need some help (data review)
Re: Need some help (data review)
_________________
| Humidifier | ||||
 | ||||
| Additional Comments: Alternate masks: Mirage Quattro Full Face Mask and Mirage Quattro FX Full Face Mask | ||||
-
justbreathe

- Posts: 134
- Joined: Sat Jul 02, 2011 5:17 am
- Location: Charlotte, NC
Re: Need some help (data review)
ASV titration is scheduled for this Sunday night. The lower pressure has not helped much. I am now having more obstructive apnea events. sometimes I feel like I can't breathe.
Strange thing is I feel better than I did before starting CPCP. Even with my current numbers they are about 50% of what they were during my first sleep study. The nurse told me that on ASV I can't be looking at the data and changing things or I will mess up my brain. I told her if I had waited for them to download my data in September for my appointment, no one would know about my high number of centrals. She said just don't be doing that and good luck on your asv titration.
I am expecting their normal two week turn around before sleep doctor reads my sleep study. Then wait for DME to order an asv. They do not keep any in stock.
Strange thing is I feel better than I did before starting CPCP. Even with my current numbers they are about 50% of what they were during my first sleep study. The nurse told me that on ASV I can't be looking at the data and changing things or I will mess up my brain. I told her if I had waited for them to download my data in September for my appointment, no one would know about my high number of centrals. She said just don't be doing that and good luck on your asv titration.
I am expecting their normal two week turn around before sleep doctor reads my sleep study. Then wait for DME to order an asv. They do not keep any in stock.
_________________
| Mask: Mirage Activa™ LT Nasal CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |

Re: Need some help (data review)
justbreathe wrote:ASV titration is scheduled for this Sunday night. The lower pressure has not helped much. I am now having more obstructive apnea events. sometimes I feel like I can't breathe.
Strange thing is I feel better than I did before starting CPCP. Even with my current numbers they are about 50% of what they were during my first sleep study. The nurse told me that on ASV I can't be looking at the data and changing things or I will mess up my brain. I told her if I had waited for them to download my data in September for my appointment, no one would know about my high number of centrals. She said just don't be doing that and good luck on your asv titration.
I am expecting their normal two week turn around before sleep doctor reads my sleep study. Then wait for DME to order an asv. They do not keep any in stock.
You posted: "sometimes I feel like I can't breathe". Is it while on the CPAP?
Are you still going to keep your appointment with the Pneumatologist?
As to having a sleep study on Sunday night. It happened to me. The clinic was located on the 2nd floor of a 4 floor bldg. But on Sunday nights the are vacuuming the floors there and make lots of noise. Next time if it happens I'll take ear plugs with me.
_________________
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: S9 Autoset machine; Ruby chinstrap under the mask straps; ResScan 5.6 |
see my recent set-up and Statistics:
http://i.imgur.com/TewT8G9.png
see my recent ResScan treatment results:
http://i.imgur.com/3oia0EY.png
http://i.imgur.com/QEjvlVY.png
http://i.imgur.com/TewT8G9.png
see my recent ResScan treatment results:
http://i.imgur.com/3oia0EY.png
http://i.imgur.com/QEjvlVY.png
Re: Need some help (data review)
**************************************Tsubs wrote:Hello there Justbreathe, I saw the post with your graphs and found it extremely strange that you exhibited an enormous amount of Centrals, two hypopneas, and not a single Obstructive apnea. Am curious what your latest graphs look like after the adjustments with your machine. While it may be true that a high pressure setting may be causing this, considering that your machine was set at 9 cmH20, coupled with S9's EPR, it is very unlikely. I'd almost suspect that your machine may not be working properly or at least might be misdiagnosing you. I read along the blog a suggestion for you to take the machine to your DME for examination as well. Maybe you should look into that, too.
As regards MD's, I agree that the best doctors are not necessarily the most educated ones with most letters after their names, but rather the ones that give you the best attention and concern. As such, try to exhaust all avenues first with the pulmonologist before consulting a neurologist.
Good luck on the ASV titration. I hope this resolves your issues. Keep us posted.
Regards,
Tsubs
Tsubs, you posted
As regards MD's, I agree that the best doctors are not necessarily the most educated ones with most letters after their names, but rather the ones that give you the best attention and concern. As such, try to exhaust all avenues first with the pulmonologist before consulting a neurologist.
I disagree with your above statement totally. I rather have a nasty physician who is a first class diagnostician ( most of them are nasty) than a Yiddishe Mamma.
_________________
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: S9 Autoset machine; Ruby chinstrap under the mask straps; ResScan 5.6 |
Last edited by avi123 on Wed Jul 27, 2011 3:14 pm, edited 1 time in total.
see my recent set-up and Statistics:
http://i.imgur.com/TewT8G9.png
see my recent ResScan treatment results:
http://i.imgur.com/3oia0EY.png
http://i.imgur.com/QEjvlVY.png
http://i.imgur.com/TewT8G9.png
see my recent ResScan treatment results:
http://i.imgur.com/3oia0EY.png
http://i.imgur.com/QEjvlVY.png

Re: Need some help (data review)
Actually, developing centrals even at very low pressures isn't altogether uncommon. I myself started getting them around 5-6. I know 9 seems pretty low to a lot of people here, but there's a lot of person to person variability in terms of what threshold may be problematic.Tsubs wrote:While it may be true that a high pressure setting may be causing this, considering that your machine was set at 9 cmH20, coupled with S9's EPR, it is very unlikely.
OK, that's just stupid. Yes, I absolutely agree that one shouldn't engage in dial-winging (frequent and quick changes to settings), but you absolutely should be looking at your data. And "mess up [your] brain"? Give me a break. That's so obnoxious.justbreathe wrote:The nurse told me that on ASV I can't be looking at the data and changing things or I will mess up my brain.
Everyone has different preferences here. I personally have found there to be a positive correlation between a doctor's attitude and his/her willingness to spend time looking at and considering my data and results. I've had Ivy League educated physicians misdiagnose things because they were constantly rushing to get to their next patient, and I've had doctors who went to middling schools figure out things that others didn't. I prefer the ones who take the time with me as a patient because that indicates they actually care, and that in turn is a good proxy for them wanting to get to the bottom of my issue.Tsubs / avi123 wrote: ...doctors...
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: minEPAP=4, minPS=2 |
-
justbreathe
- Posts: 134
- Joined: Sat Jul 02, 2011 5:17 am
- Location: Charlotte, NC
Re: Need some help (data review)
Yes, I will keep my appointment with the pulmonologist. He is the one sending me back for another test with the ASV.
My origional sleep study was mostly Hypopnea events. Correct me if I am wrong but they can be from a Central as well as obstructive. I don't believe my centrals are caused by the CPAP but just not corrected. I have high hopes for the ASV. I only wish someone would have noted that I was not properly treated with cpap on my original titration.
My current feeling of can't get my breath is on cpap with the lower pressure of 6. It allows more obstructive apnea events and with the chin strap I can't open my mouth and breath like I could before cpap. I had one Sunday night that was 68 seconds. I woke up and removed my mask. It was a bad feeling.
https://docs.google.com/document/d/18Ba ... t?hl=en_US
My origional sleep study was mostly Hypopnea events. Correct me if I am wrong but they can be from a Central as well as obstructive. I don't believe my centrals are caused by the CPAP but just not corrected. I have high hopes for the ASV. I only wish someone would have noted that I was not properly treated with cpap on my original titration.
My current feeling of can't get my breath is on cpap with the lower pressure of 6. It allows more obstructive apnea events and with the chin strap I can't open my mouth and breath like I could before cpap. I had one Sunday night that was 68 seconds. I woke up and removed my mask. It was a bad feeling.
https://docs.google.com/document/d/18Ba ... t?hl=en_US
_________________
| Mask: Mirage Activa™ LT Nasal CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |

{kind=link}
{kind=link}
{kind=link}
Re: Need some help (data review)
Yes, the Hyponeas can be central in nature as well as obstructive.justbreathe wrote:My origional sleep study was mostly Hypopnea events. Correct me if I am wrong but they can be from a Central as well as obstructive. I don't believe my centrals are caused by the CPAP but just not corrected.
I also think that since your centrals were present on the initial sleep study without cpap, and they fact that they were essentially unchanged while on cpap then they likely were not caused by the pressure. If you had not had any centrals at the first sleep study different discussion. But since they were there and still are present in high enough numbers for concern then the trial on a machine that is designed to help centrals is in order.
_________________
| Machine: AirCurve™ 10 VAuto BiLevel Machine with HumidAir™ Heated Humidifier |
| Additional Comments: Mask Bleep Eclipse https://bleepsleep.com/the-eclipse/ |
I may have to RISE but I refuse to SHINE.
Re: Need some help (data review)
justbreathe, about those Hypopneas that you're so concerned about see this report written about an interview with Resmed's chief designer of their Autosets, Dr Michael Berthon-Jones, to disregard all Hypopneas marked on graphs from these machines. And since the S9 Elite is similar to the S9 Autoset it should also be included.
Interview with Dr Berthon- Jones in 2002:
Why doesn’t ResMed's AutoSet respond to
hypopnoea?
When you are lying quietly awake, or when you
first go to sleep, or when you are dreaming, you
can have hypopneas (reductions in the depth of
breathing) which are nothing to do with the state of
the airway. For example if you sigh, which you do
every few minutes, you usually have a hypopnea
immediately afterwards. This can also happen if
you have just rolled over and are getting settled, or
if you are dreaming. And the annoying thing is that
when you are on CPAP, this tendency to have what
are called central hypopneas - hypopneas that are
nothing to do with the state of the airway - is
increased. If you make an automatic CPAP device
that responds to hypopneas, you will put the
pressure up to the maximum while the patient is
awake.
Do you think there is a misconception clinically
that all hypopneas should be treated ?
For simple obstructive sleep apnea, central
hypopneas should not be treated. They are not a
disease. Everyone has them. And they don’t go
away with CPAP.
There is a rare and important exception: central
hypopneas due to heart disease. This is called
Cheyne-Stokes breathing. CPAP does help with
that.
p.s.
1) when I put a chinstrap on I got rid of it fast. why don't you take a look at Fisher and Paykel full face masks #431 and #432.
2) Why would you not change the pressure on the Elite on your own to 8 or 9? Wouldn't you change pressures once you get the ASV?
Interview with Dr Berthon- Jones in 2002:
Why doesn’t ResMed's AutoSet respond to
hypopnoea?
When you are lying quietly awake, or when you
first go to sleep, or when you are dreaming, you
can have hypopneas (reductions in the depth of
breathing) which are nothing to do with the state of
the airway. For example if you sigh, which you do
every few minutes, you usually have a hypopnea
immediately afterwards. This can also happen if
you have just rolled over and are getting settled, or
if you are dreaming. And the annoying thing is that
when you are on CPAP, this tendency to have what
are called central hypopneas - hypopneas that are
nothing to do with the state of the airway - is
increased. If you make an automatic CPAP device
that responds to hypopneas, you will put the
pressure up to the maximum while the patient is
awake.
Do you think there is a misconception clinically
that all hypopneas should be treated ?
For simple obstructive sleep apnea, central
hypopneas should not be treated. They are not a
disease. Everyone has them. And they don’t go
away with CPAP.
There is a rare and important exception: central
hypopneas due to heart disease. This is called
Cheyne-Stokes breathing. CPAP does help with
that.
p.s.
1) when I put a chinstrap on I got rid of it fast. why don't you take a look at Fisher and Paykel full face masks #431 and #432.
2) Why would you not change the pressure on the Elite on your own to 8 or 9? Wouldn't you change pressures once you get the ASV?
_________________
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: S9 Autoset machine; Ruby chinstrap under the mask straps; ResScan 5.6 |
see my recent set-up and Statistics:
http://i.imgur.com/TewT8G9.png
see my recent ResScan treatment results:
http://i.imgur.com/3oia0EY.png
http://i.imgur.com/QEjvlVY.png
http://i.imgur.com/TewT8G9.png
see my recent ResScan treatment results:
http://i.imgur.com/3oia0EY.png
http://i.imgur.com/QEjvlVY.png
Re: Need some help (data review)
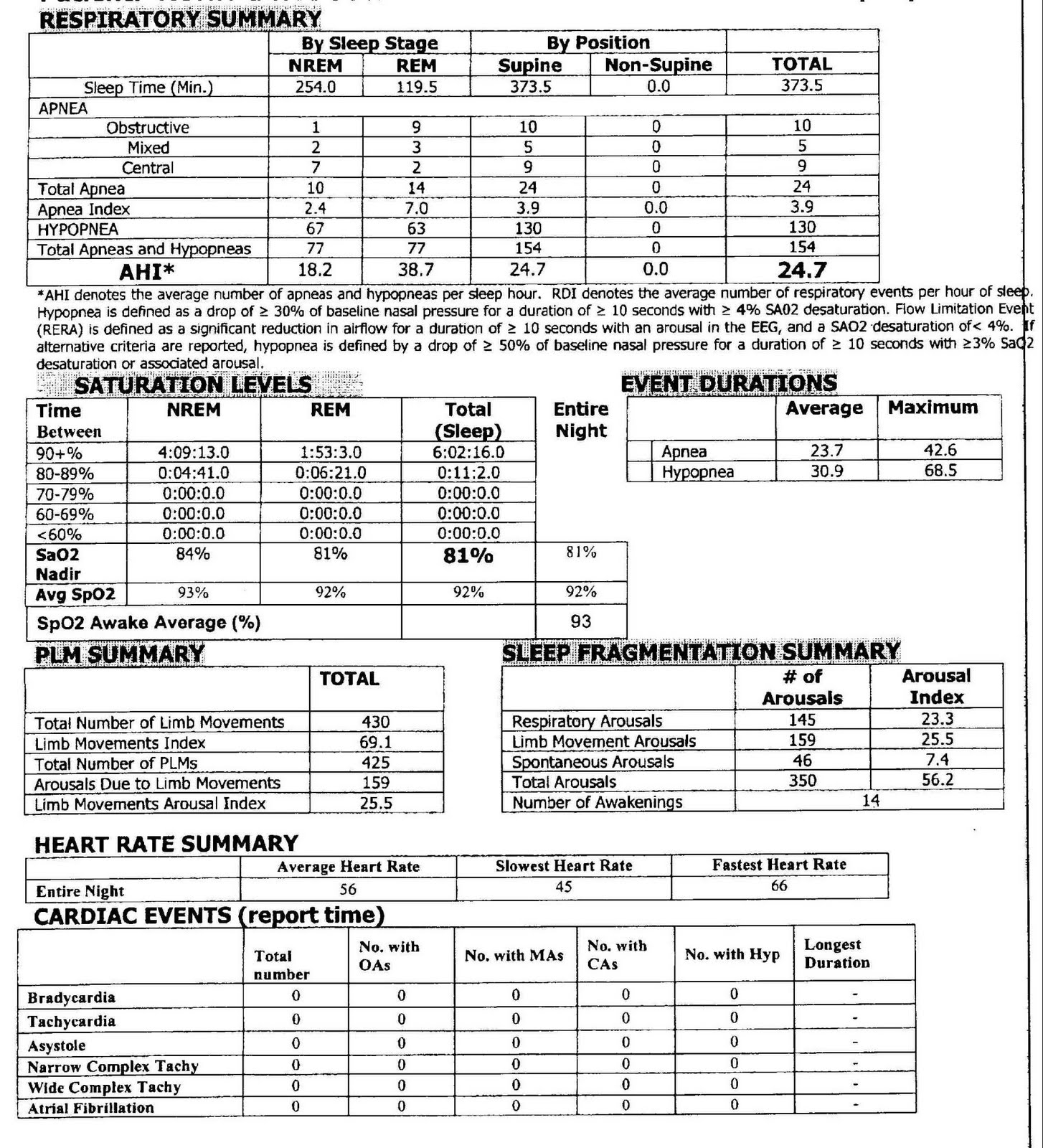
Hi Pugsy! This is possible, but to me it looks like justbreathe's centrals are much worse when on CPAP than not. In his diagnostic study, he had 9 centrals over the course of 373 minutes, which is a CA index of 1.5. It's possible many of those were during sleep onset too (we know he only had 2 during REM). That all seems fairly typical in the grand scheme of things. By contrast, he's having about an order of magnitude more CA-flagged events per hour while on CPAP. Tell me if I glossed over something too quickly in the data, but that's what has me thinking that the untreated centrals aren't too big of a problem and that this (at first blush) looks more like complex SAS.Pugsy wrote: I also think that since your centrals were present on the initial sleep study without cpap
I'm hopeful for you as well, but I also hope that you don't go into this equating high hopes with high expectations. ASV excels at certain things, but it is not a panacea. For people with traditional CSR, for example, it's wonderful. ASV is the treatment of choice for complex sleep apnea too. But, it can cause more problems too (see Paper_Nanny's thread here; she's very close to moving away from her default ASV settings and back to something more like pure CPAP). The PLMD makes for a potentially frustrating complication. AND, if you're like me and a few other posters around here, they'll get you looking wonderful in the lab, and then you'll come home and have to spend time scratching your head as to why you're still having events. All of the above is why I urge you not to be disappointed if the ASV isn't the end of your journey. I hope for your sake that it is! Fortunately, even if it isn't, folks here can help.justbreathe wrote:I have high hopes for the ASV.
Happened to me too. My CPAP night was awful, and that was clearly obvious from the numbers. Unfortunately, it took me a year of jerking with medical people until my ASV titration. Once I started learning, I was pretty mortified by it all. You're ahead of the curve in that respect.justbreathe wrote:I only wish someone would have noted that I was not properly treated with cpap on my original titration.
I'm not surprised. I use the same mask as you (Swift LT) with my ASV, and my starting exhalation pressure (EPAP) is 4. I too feel like I'm suffocating on it, which is why I keep my minimum PS (pressure support -- i.e., the difference between IPAP and EPAP) much higher -- it makes it a lot more comfortable for me. And yes, PS is supposed to be a therapeutic setting, not a patient comfort setting...but in my case, it makes the Swift LT mask tolerable. For what it's worth, I have no problems feeling suffocated at low pressures when using my full face mask.justbreathe wrote:My current feeling of can't get my breath is on cpap with the lower pressure of 6.
If you want to continue using your Swift LT mask (and I think it's an excellent choice for the record), be sure to take it in with you to your titration. Ideally, you do NOT want to be titrated on a FFM if a nasal pillow is what you'll use at home.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: minEPAP=4, minPS=2 |
Re: Need some help (data review)
You are correct. I misread the 9 and thought it was hourly index. So my mistake.BrianinTN wrote:He had 9 centrals over the course of 373 minutes, which is a CA index of 1.5. It's possible many of those were during sleep onset too (we know he only had 2 during REM).
If it were me I would rather have it as high hourly on initial sleep study. I would be afraid that I might end up in the same boat you are in. We both know that boat isn't a fun boat. I would also think that the sleep study tech would have already discounted any centrals that might have been sleep onset centrals. I would have to trust them to know the difference. They have that data right in front of them.
So to OP, please disregard my previous comment about same number of centrals pre cpap and post cpap. It higher with cpap. You are doing the right thing getting it re-evaluated with the ASV titration no matter when it is worse though.
_________________
| Machine: AirCurve™ 10 VAuto BiLevel Machine with HumidAir™ Heated Humidifier |
| Additional Comments: Mask Bleep Eclipse https://bleepsleep.com/the-eclipse/ |
I may have to RISE but I refuse to SHINE.
Re: Need some help (data review)
justbreathe, by any chance could you post a Flow graph from your S9 Elite at low speed?
I would be interested to look at the individual respiration cycles immediately after a Central Apnea flag.
Something like this:

If you agree I could then PM you step by step how I do it.
https://docs.google.com/viewer?pid=expl ... er=1&w=664
I would be interested to look at the individual respiration cycles immediately after a Central Apnea flag.
Something like this:
If you agree I could then PM you step by step how I do it.
https://docs.google.com/viewer?pid=expl ... er=1&w=664
_________________
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: S9 Autoset machine; Ruby chinstrap under the mask straps; ResScan 5.6 |
Last edited by avi123 on Thu Jul 28, 2011 6:36 am, edited 1 time in total.
see my recent set-up and Statistics:
http://i.imgur.com/TewT8G9.png
see my recent ResScan treatment results:
http://i.imgur.com/3oia0EY.png
http://i.imgur.com/QEjvlVY.png
http://i.imgur.com/TewT8G9.png
see my recent ResScan treatment results:
http://i.imgur.com/3oia0EY.png
http://i.imgur.com/QEjvlVY.png
-
justbreathe
- Posts: 134
- Joined: Sat Jul 02, 2011 5:17 am
- Location: Charlotte, NC
Re: Need some help (data review)
How is this for a sample.

_________________
| Mask: Mirage Activa™ LT Nasal CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
-
justbreathe
- Posts: 134
- Joined: Sat Jul 02, 2011 5:17 am
- Location: Charlotte, NC
Re: Need some help (data review)
Here is another one. The wave form is all over the place. I will sleep steady for twenty min or so then this stuff starts up. Sometimes I wake up but these times it I don't think it woke me up.
_________________
| Mask: Mirage Activa™ LT Nasal CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
Last edited by justbreathe on Thu Jul 28, 2011 2:22 pm, edited 1 time in total.
Re: Need some help (data review)
I can't see any of the the two graphs. I see only an X in a box. It's possible that you did not make the Doc to be shared.
Google flags it as:
"Your search - https://docs.google.com/viewer?pid=explorer&srcid ... - did not match any documents."
Sorry, we are unable to retrieve the document for viewing or you don't have permission to view the document.
*******************************
I sent you a pm how I get the ResScan Flow and Events traces at hi speed to see each individual cycle. If you do it we could then look for Schein- Stoke breathing. Total time scale in the following flow and events traces is one minute:

Google flags it as:
"Your search - https://docs.google.com/viewer?pid=explorer&srcid ... - did not match any documents."
Sorry, we are unable to retrieve the document for viewing or you don't have permission to view the document.
*******************************
I sent you a pm how I get the ResScan Flow and Events traces at hi speed to see each individual cycle. If you do it we could then look for Schein- Stoke breathing. Total time scale in the following flow and events traces is one minute:
_________________
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: S9 Autoset machine; Ruby chinstrap under the mask straps; ResScan 5.6 |
see my recent set-up and Statistics:
http://i.imgur.com/TewT8G9.png
see my recent ResScan treatment results:
http://i.imgur.com/3oia0EY.png
http://i.imgur.com/QEjvlVY.png
http://i.imgur.com/TewT8G9.png
see my recent ResScan treatment results:
http://i.imgur.com/3oia0EY.png
http://i.imgur.com/QEjvlVY.png
-
justbreathe
- Posts: 134
- Joined: Sat Jul 02, 2011 5:17 am
- Location: Charlotte, NC
Re: Need some help (data review)
Don't know why they did not show up before. Anyway take another look at the waves I posted above.
_________________
| Mask: Mirage Activa™ LT Nasal CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |