NotMuffy wrote:Interestingly, resolution of the sleep-related breathing instability associated with CompSAS usually occurs after about a month, so this seems quite the reverse of what should be happening.
Yes, it does. <another big sigh> At one time, I was one of those people who systemactically disobeyed the unspoken rules of social behaviour. If someone had been watching me at that time in my life, the observer would have said, "How interesting! What she is doing
seems quite the reverse of what should be happening." I wonder now if I went so far with that that on some deep, subconscious level, I decided This Is The Way To Be. And now, my body itself does things that seem
quite the reverse of what should be happening.
[I wish I could embed little sound clips into my posts. "I don't know how to stop, no I don't know how to stop" Peter Gabriel, No Self Control...]
Seriously, though... This isn't the first time medical issues, drug reactions, etc. have been labelled as seemingly quite the reverse of what should be happening. I don't know why.
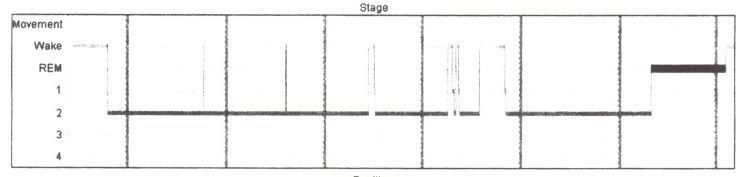
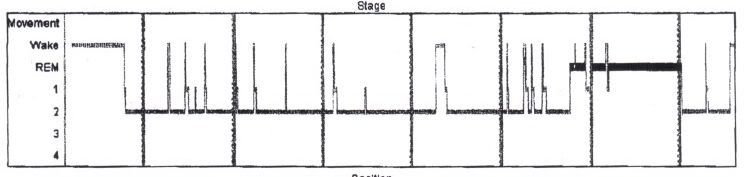
NotMuffy wrote:Your sleep architecture on both sleep studies appear to be heavily influenced by medication effect. Do you have a medication list and a timeline of everything back to the first sleep study?
MSD and my neurologist both concluded that drug effect was not an issue. However, I am not sure I trust their opinions on this one. During the appointment with Kurt the Neurologist to discuss just this issue, he said, "I don't know anything about MS that you couldn't find out on your own" and "If you have a sophisticated patient with access to the internet, they could find out more than I could about this, given the limited amount of time available." That was after making me wait for fifteen minutes while he discussed paint colours with the building maintenance people.
Yes, I do have a medication list and timeline from back when both studies were done. I will post it if that would be helpful to you.
Deborah