






Emilia has posted this DeVilbiss link in another thread - it worthy of having a thread of its own:
http://www.devilbisshealthcare.com/file ... T-2089.pdf
DeVilbiss has always been good at sharing the important information about auto adjusting machines and this document is in the same tradition. They had webinars here: http://www.devilbissclinicaleducation.com/ondemand - but "starting Jan 1st 2011 all webinars are now put on hold for renewal")
A very good introduction to auto adjusting machines - should be read by anyone who's attempting to understand this kind of therapy.
About APAP and algorithms - document from DeVilbiss
About APAP and algorithms - document from DeVilbiss
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023

Re: About APAP and algorithms - document from DeVilbiss
good idea ozij! We can keep it bumped for a while. Folks should download the pdf from the link and save it.
Yes, that blue eyed beauty is my cat! He is a seal point, bi-color Ragdoll. I adopted him in '08 from folks who could no longer care for him. He is a joy and makes me smile each and every day.

Re: About APAP and algorithms - document from DeVilbiss
Good info!
Slanted heavily toward DeVilbiss, but that's to be expected. Still lots of history and explanation.
Slanted heavily toward DeVilbiss, but that's to be expected. Still lots of history and explanation.
_________________
| Machine | Mask | Humidifier | ||
 |  |  | ||
| Additional Comments: 11-14 cmH2O | ||||
The OSA patient died quietly in his sleep.
Unlike his passengers who died screaming as the car went over the cliff...
Unlike his passengers who died screaming as the car went over the cliff...
-
M.D.Hosehead

- Posts: 742
- Joined: Thu Jun 24, 2010 7:16 pm
- Location: Kansas
Re: About APAP and algorithms - document from DeVilbiss
Thanks for bumping this, O. It's a valuable resource.
I'm thinking DeVilbiss is the only PAP manufacturer that regards the users of its products as other than imbeciles to be ignored.
The above paper gave me numerical understanding of something I had understood only in a general way: LEAKS DON'T HAVE TO BE ZERO. The DeVilbiss machine's algorithms still work with leaks up to 95 l/m. Try to find that kind of specific information from any other manufacturer and see how far you get.
Also, the paper says the prescribed pressure can be maintained with leak rates even higher than 95 l/m, though the ability to interpret the pressure and flow numbers is lost. I wonder whether there's a different, lower, threshold leak rate beyond which the tallys (of apneas, hypopneas, etc.) and indices, and therefore the reports, become unreliable.
Another question: the DeVilbiss algorithm uses detection of expiratory puffs and snoring to adjust—or to not adjust—pressure. But how useful are these with a FFM?
I hope someone from DeVilbiss discovers this thread and responds.
I'm thinking DeVilbiss is the only PAP manufacturer that regards the users of its products as other than imbeciles to be ignored.
The above paper gave me numerical understanding of something I had understood only in a general way: LEAKS DON'T HAVE TO BE ZERO. The DeVilbiss machine's algorithms still work with leaks up to 95 l/m. Try to find that kind of specific information from any other manufacturer and see how far you get.
Also, the paper says the prescribed pressure can be maintained with leak rates even higher than 95 l/m, though the ability to interpret the pressure and flow numbers is lost. I wonder whether there's a different, lower, threshold leak rate beyond which the tallys (of apneas, hypopneas, etc.) and indices, and therefore the reports, become unreliable.
Another question: the DeVilbiss algorithm uses detection of expiratory puffs and snoring to adjust—or to not adjust—pressure. But how useful are these with a FFM?
I hope someone from DeVilbiss discovers this thread and responds.
_________________
| Mask: Forma Full Face CPAP Mask with Headgear |
| Additional Comments: MaxIPAP 15; MinEPAP 10; Also use Optilife nasal pillow mask with tape |
-
Jayjonbeach

- Posts: 133
- Joined: Sun Aug 15, 2010 9:04 am
- Location: Mississauga
Re: About APAP and algorithms - document from DeVilbiss
The BIG problem with Devilbiss is not only is their algorithm less agressive than others, they are also lumping snoring and flow limitation together which is a HUGE mistake IMO and I know many people that have knowledge on the subject I have talked to agree on this.
Right on the bottom of page 3, Devilbiss address's this by saying there is conflicting information, to me it is more of a LACK of information on their part:
Snoring versus Flow Limitation
Snoring and flow limitation are similar in that both may occur prior to obstructive apneas and/or
hypopneas. All Autotitrating PAPs are proactively programmed to increase pressure in response to
snores or flow limitations to prevent the occurrence of obstructive apneas and hypopneas. There is
conflicting evidence as to which parameter allows the earliest response.
Yes sometimes someone will experience these both together, sometimes being the key word and maybe seldom being more accurate (depending on the person of course). At any rate, why would a company LIMIT themselves to adjusting pressure on just ONE of these precursors? Right, there is no good reason, which is why other manufacturers allow the machine to respond to EITHER occurance.
When I look at my charts (now and especially before when on just CPAP therapy) very often (notice the difference here from seldom...) Flow limitation is the VERY FIRST sign of trouble AND there is NO snoring at the same time. Like we say in the stock market, the charts don't lie, this is VERY clear.
For example on CPAP therapy, often between 2 - 3am I would likely enter REM sleep and my airway would become more relaxed. This first shows as FLOW LIMITATION which gets progressively worse over a matter of a couple of minutes, then a whole whack of apneas, like 10 apneas in 5 minutes all obstructive, and of course a CPAP machine does NOTHING to prevent this (and Devilbiss APAP users will have to wait for an apnea or snore event to occur).
With a Resmed S9 APAP machine, this repetitive ugly process night after night is almost completely avoided. At the first signs of Flow Limitation it ups the pressure, if it is not corrected it ups it more and will keep doing that until Flow resumes a normal pattern, and this often avoids the REM issue completely (its not foolproof but I see it working MOST of the time and even if an apnea slips in it is one instead of TEN!). It is also an agressive response depending on severity of event, if the flow is quite bad it CRANKS the pressure immediately and doesn't fart around which is great if your airway is closing, unlike Devilbiss (there was a 3rd party study with charts done on this and it showed that Devilbiss had the least aggressive response out of 5 manufactures).
Devilbiss responding to Flow Limitation? Nope sorry. Either you have to snore or have an apnea before it does anything and that is not a road I wanted to go down. YMMV When buying a machine ask yourself if this is something you are willing to accept, I could have bought one for half the price but to me it wasn't worth it, again, YMMV but my charts are VERY clear about this.
I'm not saying it is a bad machine, but I do think ignoring Flow Limitation was clearly a bad choice on their part and won't be surprised if they change this going forward. I know there is a Devilbiss Rep in these forums, please feel free to comment if so inclined.
Right on the bottom of page 3, Devilbiss address's this by saying there is conflicting information, to me it is more of a LACK of information on their part:
Snoring versus Flow Limitation
Snoring and flow limitation are similar in that both may occur prior to obstructive apneas and/or
hypopneas. All Autotitrating PAPs are proactively programmed to increase pressure in response to
snores or flow limitations to prevent the occurrence of obstructive apneas and hypopneas. There is
conflicting evidence as to which parameter allows the earliest response.
Yes sometimes someone will experience these both together, sometimes being the key word and maybe seldom being more accurate (depending on the person of course). At any rate, why would a company LIMIT themselves to adjusting pressure on just ONE of these precursors? Right, there is no good reason, which is why other manufacturers allow the machine to respond to EITHER occurance.
When I look at my charts (now and especially before when on just CPAP therapy) very often (notice the difference here from seldom...) Flow limitation is the VERY FIRST sign of trouble AND there is NO snoring at the same time. Like we say in the stock market, the charts don't lie, this is VERY clear.
For example on CPAP therapy, often between 2 - 3am I would likely enter REM sleep and my airway would become more relaxed. This first shows as FLOW LIMITATION which gets progressively worse over a matter of a couple of minutes, then a whole whack of apneas, like 10 apneas in 5 minutes all obstructive, and of course a CPAP machine does NOTHING to prevent this (and Devilbiss APAP users will have to wait for an apnea or snore event to occur).
With a Resmed S9 APAP machine, this repetitive ugly process night after night is almost completely avoided. At the first signs of Flow Limitation it ups the pressure, if it is not corrected it ups it more and will keep doing that until Flow resumes a normal pattern, and this often avoids the REM issue completely (its not foolproof but I see it working MOST of the time and even if an apnea slips in it is one instead of TEN!). It is also an agressive response depending on severity of event, if the flow is quite bad it CRANKS the pressure immediately and doesn't fart around which is great if your airway is closing, unlike Devilbiss (there was a 3rd party study with charts done on this and it showed that Devilbiss had the least aggressive response out of 5 manufactures).
Devilbiss responding to Flow Limitation? Nope sorry. Either you have to snore or have an apnea before it does anything and that is not a road I wanted to go down. YMMV When buying a machine ask yourself if this is something you are willing to accept, I could have bought one for half the price but to me it wasn't worth it, again, YMMV but my charts are VERY clear about this.
I'm not saying it is a bad machine, but I do think ignoring Flow Limitation was clearly a bad choice on their part and won't be surprised if they change this going forward. I know there is a Devilbiss Rep in these forums, please feel free to comment if so inclined.
_________________
| Mask: Quattro™ FX Full Face CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Software is actually 3.11. Curious about Oxygen and whether I might need it or just want it. |
Tired of being tired for 20 years running, hoping this is the answer...
-
Jayjonbeach
- Posts: 133
- Joined: Sun Aug 15, 2010 9:04 am
- Location: Mississauga
Re: About APAP and algorithms - document from DeVilbiss
Here is some more juicy info from their own document, middle of page 6 and top of page 7:
Event Set Measurement™
DeVilbiss uses its unique Event Set Measurement to increase the algorithm’s ability to identify
abnormal breathing events and to determine appropriate response speeds. The algorithm uses
a series of 6 one-minute windows, collectively referred to as the Event Set, to deliver a
comprehensive view of the most recent six minutes of therapy.
Algorithm
DeVilbiss, in collaboration with a clinical advisory team, developed the AutoAdjust algorithm
including the Event Set Measurement. The Event Set Measurement is unique to the DeVilbiss
AutoAdjust and allows our devices to make pressure changes every minute and in varying
increments which can improve patient comfort and reduce arousals caused by increasing
pressure based on a single event, overreacting to artifacts and noise in the signal or decreasing
pressures before breathing has stabilized.
This likely explains why their algorithm is LESS Aggressive than other manufactures, they are looking at a SIX minute window to determine their adjustments! YIKES!
They say, " which can improve patient comfort and reduce arousals caused by increasing
pressure based on a single event, overreacting to artifacts and noise in the signal or decreasing pressures before breathing has stabilized".
Ahhhh this is at the cost of letting more apneas happen. Again I refer to the 3rd party study which I dont have the link for just now maybe someone will post it, their responses are slower and less aggressive (less rise in pressure) which sure MIGHT be more comfortable for some, LESS for others if they are choking and need a burst of pressure to open their airway. So they admit this in the quotes above pointing to comfort.
Another quote" There are two reasons for responding less quickly to breathing events: fast response times wake
patients or bring them to partial arousal; and fast response times have a greater percentage of
false responses. The AutoAdjust mimics sleep lab manual procedures by initiating a moderate and
controlled response to breathing events.
While this is undoubtable somewhat true and explains their reasoning for what they did, they also fail to mention, "APNEAS WILL cause arousals"
Eegads, page 8: Snores, as precursors to apneas and hypopneas, are treated aggressively. Pressure
increases up to 1 cmH2O per minute until the mix of snores, apneas and hypopneas
no longer warrants a higher pressure. After breathing stabilizes, pressure decreases
0.6 cmH2O every 6 minutes until it reaches the lowest pressure setting or until
additional breathing events warrant a further response.
"AGGRESSIVELY"??? LOL A whole 1cm per minute, oh my, again I would have choked nearly to death by the time it got up to a pressure that would actually open my airway in REM sleep. They also use this same method for Obstructive Apneas and I quote" If apnea density trends meet specific criteria, the algorithm increases the pressure
up to 1 cmH2O per minute until the density trending no longer warrants increased
pressure. WOW, just wow.
Clearly those people having arousal issues with APAP could possibly benfit here, others, not so much IMO.
Again comparing Resmed and I could be wrong here as I am going by memory, they use a BREATH by breath measurement, and I think it is your last 5 or 6 breaths NOT last 5 or 6 minutes!!! Hell in 6 minutes I can easily have 10 apneas and do if my pressure is not increased high enough and fast enough. I know the burst of air at the right time is working for me, my pressure can jump FIVE cm if it needs to (THATS aggressive folks) to open my airway or prevent it from closing i the first place and I see it clearly works for me, YMMV as always.
Event Set Measurement™
DeVilbiss uses its unique Event Set Measurement to increase the algorithm’s ability to identify
abnormal breathing events and to determine appropriate response speeds. The algorithm uses
a series of 6 one-minute windows, collectively referred to as the Event Set, to deliver a
comprehensive view of the most recent six minutes of therapy.
Algorithm
DeVilbiss, in collaboration with a clinical advisory team, developed the AutoAdjust algorithm
including the Event Set Measurement. The Event Set Measurement is unique to the DeVilbiss
AutoAdjust and allows our devices to make pressure changes every minute and in varying
increments which can improve patient comfort and reduce arousals caused by increasing
pressure based on a single event, overreacting to artifacts and noise in the signal or decreasing
pressures before breathing has stabilized.
This likely explains why their algorithm is LESS Aggressive than other manufactures, they are looking at a SIX minute window to determine their adjustments! YIKES!
They say, " which can improve patient comfort and reduce arousals caused by increasing
pressure based on a single event, overreacting to artifacts and noise in the signal or decreasing pressures before breathing has stabilized".
Ahhhh this is at the cost of letting more apneas happen. Again I refer to the 3rd party study which I dont have the link for just now maybe someone will post it, their responses are slower and less aggressive (less rise in pressure) which sure MIGHT be more comfortable for some, LESS for others if they are choking and need a burst of pressure to open their airway. So they admit this in the quotes above pointing to comfort.
Another quote" There are two reasons for responding less quickly to breathing events: fast response times wake
patients or bring them to partial arousal; and fast response times have a greater percentage of
false responses. The AutoAdjust mimics sleep lab manual procedures by initiating a moderate and
controlled response to breathing events.
While this is undoubtable somewhat true and explains their reasoning for what they did, they also fail to mention, "APNEAS WILL cause arousals"
Eegads, page 8: Snores, as precursors to apneas and hypopneas, are treated aggressively. Pressure
increases up to 1 cmH2O per minute until the mix of snores, apneas and hypopneas
no longer warrants a higher pressure. After breathing stabilizes, pressure decreases
0.6 cmH2O every 6 minutes until it reaches the lowest pressure setting or until
additional breathing events warrant a further response.
"AGGRESSIVELY"??? LOL A whole 1cm per minute, oh my, again I would have choked nearly to death by the time it got up to a pressure that would actually open my airway in REM sleep. They also use this same method for Obstructive Apneas and I quote" If apnea density trends meet specific criteria, the algorithm increases the pressure
up to 1 cmH2O per minute until the density trending no longer warrants increased
pressure. WOW, just wow.
Clearly those people having arousal issues with APAP could possibly benfit here, others, not so much IMO.
Again comparing Resmed and I could be wrong here as I am going by memory, they use a BREATH by breath measurement, and I think it is your last 5 or 6 breaths NOT last 5 or 6 minutes!!! Hell in 6 minutes I can easily have 10 apneas and do if my pressure is not increased high enough and fast enough. I know the burst of air at the right time is working for me, my pressure can jump FIVE cm if it needs to (THATS aggressive folks) to open my airway or prevent it from closing i the first place and I see it clearly works for me, YMMV as always.
_________________
| Mask: Quattro™ FX Full Face CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Software is actually 3.11. Curious about Oxygen and whether I might need it or just want it. |
Tired of being tired for 20 years running, hoping this is the answer...

Re: About APAP and algorithms - document from DeVilbiss
I would respectfully submit that if your present machine settings still allow "choking" that "need(s) a burst of pressure to open their airway", then the machine is set up incorrectly.Jayjonbeach wrote:Ahhhh this is at the cost of letting more apneas happen. Again I refer to the 3rd party study which I dont have the link for just now maybe someone will post it, their responses are slower and less aggressive (less rise in pressure) which sure MIGHT be more comfortable for some, LESS for others if they are choking and need a burst of pressure to open their airway. "AGGRESSIVELY"??? LOL A whole 1cm per minute, oh my, again I would have choked nearly to death by the time it got up to a pressure that would actually open my airway in REM sleep. They also use this same method for Obstructive Apneas and I quote" If apnea density trends meet specific criteria, the algorithm increases the pressure up to 1 cmH2O per minute until the density trending no longer warrants increased pressure. WOW, just wow.
I could see how a machine set "wide open" (4-20) might have trouble keeping up with events if response time were slow, but if opening pressure were set high enough to attack the great majority of events (which it should be), then there shouldn't be a lot of "choking-level" events.
Further, one must also look at the time required to return to baseline pressure. If a rapid-increase machine is also a rapid-decrease machine, and the range is set too wide, then the net result is probably worse that a slow-increase, slow-decrease machine.
"Don't Blame Me...You Took the Red Pill..."
Re: About APAP and algorithms - document from DeVilbiss
A good gauge might be to look at FLs and hypopneas.NotMuffy wrote:Further, one must also look at the time required to return to baseline pressure. If a rapid-increase machine is also a rapid-decrease machine, and the range is set too wide, then the net result is probably worse that a slow-increase, slow-decrease machine.
In the case of hypopneas:
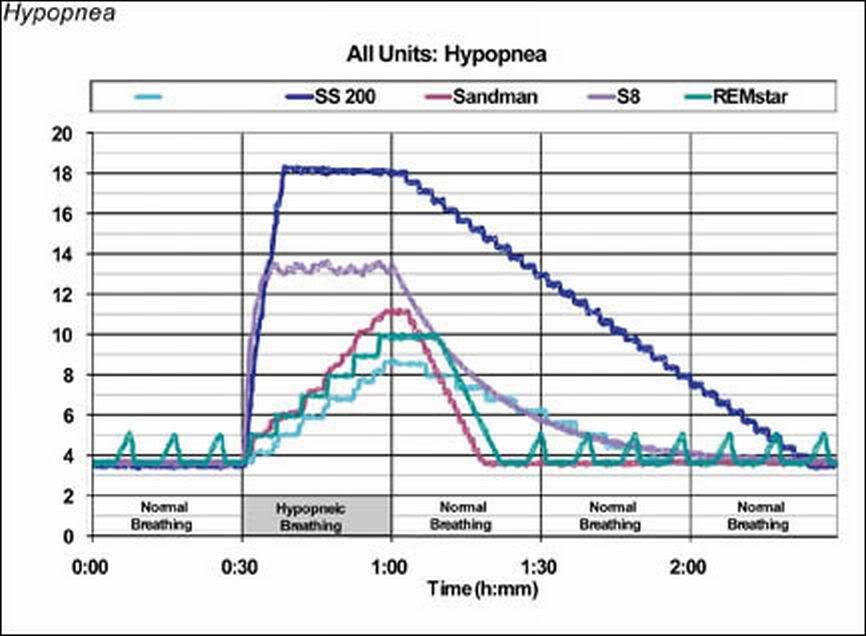
Algorithm Comparison
If the night is about 420 minutes long, I don't see where a 6-minute acclimitization period would be a deal-breaker, and I think one thing this slide dramatically shows is that one should really know just what the heck they're trying to treat before they try to treat it.
"Don't Blame Me...You Took the Red Pill..."
Re: About APAP and algorithms - document from DeVilbiss
DeVilbiss is that turquoise track (see color on the left) with the name missing.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
-
AHI_Killer
Re: About APAP and algorithms - document from DeVilbiss
IO nominate this for Thread of the Year, 2011. Excellent information, thanks everyone! Makes me think I should ditch my IntelliPap and try an S9 since I'm still not happy with my therapy after a year (lots of awakenings during REM, may be due to delayed, conservative response by the IntelliPAP and it's failure to preempt events by responding to flow limitations).
-
DeVilbiss Marketing

- Posts: 116
- Joined: Sat Mar 28, 2009 9:35 am
Re: About APAP and algorithms - document from DeVilbiss
Most auto devices should be able to accomodate typical mask leak flow rates (30/40 LPM). The DeVilbiss AutoAdjust algorithm will continue to detect and report leaks up to 95 LPM. When a leak above 95 LPM is detected, your efficacy data will not report events other than a high leak until the leak is resolved.M.D.Hosehead wrote:Thanks for bumping this, O. It's a valuable resource.
Also, the paper says the prescribed pressure can be maintained with leak rates even higher than 95 l/m, though the ability to interpret the pressure and flow numbers is lost. I wonder whether there's a different, lower, threshold leak rate beyond which the tallys (of apneas, hypopneas, etc.) and indices, and therefore the reports, become unreliable.
Another question: the DeVilbiss algorithm uses detection of expiratory puffs and snoring to adjust—or to not adjust—pressure. But how useful are these with a FFM?
Snoring is a viable parameter for the AutoAdjust to detect and respond to with a FFM. For nasal interface users, the EPI is an indicator that a FFM, chin strap or oral nasal interface may be required. EPI is not common with a FFM - although there are instances of this occuring.
DeVilbiss is interested in your needs and will continue to monitor this message board in order to continually improve the solutions we provide.
Re: About APAP and algorithms - document from DeVilbiss
Don't all manufacturers claim their machines should be run wide open? Do any manufacturers actually recommend raising the minimum like that, even though we know that works best?NotMuffy wrote: . . . I could see how a machine set "wide open" (4-20) might have trouble keeping up with events if response time were slow, but if opening pressure were set high enough to attack the great majority of events (which it should be) . . .
I know that patients have found on their own that setting a machine that way (with EPAP within a cm or two of the pressure needed to address apnea events) will decrease their AHI, but I thought that was just a dial-wingin'-patient tactic, not a tactic recommended by manufacturers, who all (as far as I know) claim their autos need no manual titration or patient tweaking for optimal performance.
Or maybe I have that all wrong. I honestly don't know.
-
DeVilbiss Marketing
- Posts: 116
- Joined: Sat Mar 28, 2009 9:35 am
Re: About APAP and algorithms - document from DeVilbiss
Achieving the lowest pressure to maintain airway patency is at the foundation of the DeVilbiss AutoAdjust algorithm.
The benchtop testing cited was conducted by Valley Inspired Products and published in Sleep Review http://www.sleepreviewmag.com/issues/ar ... -09_02.asp and RT Magazine http://www.rtmagazine.com/issues/articl ... -08_05.asp and did not include a snore signal. As such we contacted VIP, provided them with a snore box and asked them to re-conduct the testing. Their results indicated that “the snore signal did have a significant impact on the response” and “yielded a more rapid pressure response,”
[IMG=http://www.image-share.com/upload/508/102m.jpg]
We understand that some may require a more aggressive response to apneas and hypopneas; as such we are the only manufacturer that accommodates adjustments to the definition of these events. To increase sensitivity, or respond more aggressively to apneas, the apnea percentage should be adjusted toward 20% and/or the duration toward 6 seconds. To increase sensitivity, or respond more aggressively to hypopneas, the hypopnea percentage can be adjusted toward 30% and/or the duration toward 6 seconds.
It should be noted that every 60 seconds, the DeVilbiss algorithm decides whether to increase, decrease, or maintain the current therapy pressure. The Event Set Measurement is used for event trending.
At the end of the night – we want folks to feel well and we appreciate input and discussions concerning our technology.
The benchtop testing cited was conducted by Valley Inspired Products and published in Sleep Review http://www.sleepreviewmag.com/issues/ar ... -09_02.asp and RT Magazine http://www.rtmagazine.com/issues/articl ... -08_05.asp and did not include a snore signal. As such we contacted VIP, provided them with a snore box and asked them to re-conduct the testing. Their results indicated that “the snore signal did have a significant impact on the response” and “yielded a more rapid pressure response,”
[IMG=http://www.image-share.com/upload/508/102m.jpg]
We understand that some may require a more aggressive response to apneas and hypopneas; as such we are the only manufacturer that accommodates adjustments to the definition of these events. To increase sensitivity, or respond more aggressively to apneas, the apnea percentage should be adjusted toward 20% and/or the duration toward 6 seconds. To increase sensitivity, or respond more aggressively to hypopneas, the hypopnea percentage can be adjusted toward 30% and/or the duration toward 6 seconds.
It should be noted that every 60 seconds, the DeVilbiss algorithm decides whether to increase, decrease, or maintain the current therapy pressure. The Event Set Measurement is used for event trending.
At the end of the night – we want folks to feel well and we appreciate input and discussions concerning our technology.
Re: About APAP and algorithms - document from DeVilbiss
Back in Nov. 2009 we had a discussion of
Back in November 2009 DoriC brought that article to our attention, and we had a long discussion of it. This was my comment on that thread, (edited for the usual typos...)DeVilbiss Marketing wrote:The benchtop testing cited was conducted by Valley Inspired Products and published in Sleep Review http://www.sleepreviewmag.com/issues/ar ... -09_02.asp and RT Magazine http://www.rtmagazine.com/issues/articl ... -08_05.asp and did not include a snore signal. As such we contacted VIP, provided them with a snore box and asked them to re-conduct the testing. Their results indicated that “the snore signal did have a significant impact on the response” and “yielded a more rapid pressure response,”
At the really nice part is that this type of study is making the manufacturers discuss their algorithms openly - something they refrained from doing in the past.ozij wrote:Thanks, Dori!The reason for the DeVilbiss's lack of response is that - ironically - the apnea signal selected by the researchers is one of close to 100% reduction in flow, which happens to fall within the DeVilbiss's "oh my gosh, this is a central apnea, I'm not responding to that" category.Sandman, and S8 units all increased pressure above 10 cm H2O, suggesting a pressure response to other nonapneic events present in the signal. The intelliPAP (DeVilbiss) unit responded less quickly, achieving a maximum therapy pressure of 5.5 cm H2O by the end of the 30-minute apnea session.
I know this, because in their previous reports, the authors showed the signals.
The breathing pattern thrown at the machines can be seen here "Created Unequal" McCoy and Eiken 2006 - a previous version of the benchmarks, but the breathing patterns were not changed:
This actually the first such benchmark comparison in which the authors take into a account a point made by -SWS years ago: The mahcines in this simulation are not getting any response from the mechanical device connected to them. And this is the first time (IIRC) that the results are analysed within this proper context.
Science is finally catching up with members of this forum...

That's when they want to sell them as the autotitrating magic bullet that will save insurance companys the time and money invovlved in PSG's. And the, people are supposed to moved to the machine's recommended 90th or 95th percentile pressure, at fixed pressure.jnk wrote:NotMuffy wrote:
. . . I could see how a machine set "wide open" (4-20) might have trouble keeping up with events if response time were slow, but if opening pressure were set high enough to attack the great majority of events (which it should be) . . .
Don't all manufacturers claim their machines should be run wide open? Do any manufacturers actually recommend raising the minimum like that, even though we know that works best?
Hi there, Bob3000,long time no see! Congratutlation on changing your mind.AHI_Killer, also posted as Bob3000 wrote:IO nominate this for Thread of the Year, 2011. Excellent information, thanks everyone! Makes me think I should ditch my IntelliPap and try an S9 since I'm still not happy with my therapy after a year (lots of awakenings during REM, may be due to delayed, conservative response by the IntelliPAP and it's failure to preempt events by responding to flow limitations).
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
-
Guest
Re: About APAP and algorithms - document from DeVilbiss
Yes, I was wrong in my original conclusion, which is yet further validation of my policy to try to always keep an open mind - if I had stopped considering new information after reaching my original conclusion, I would never have learned just how different each aPAP algorithm really is. Again, thanks for this thread. Fingers crossed that my S9 will work for me better than the intellipap. I think I am just a poor candidate for the intellipap (which is in general an excellent machine) because (1) I often mouth breath and use only FFM's which may throws things off a bit (eg no exhalation puffs), (2) I never snore, with or without CPAP (site note: this is part of the reason for my ~8 year delayed diagnosis and the reason I had to diagnose myself, *then* convince my doc a PSG was warranted which confirmed my dx) so again, that throws the algorithm off and (3) I have lots and lots of hypopneas, but no apneas, either by intellipap's definition OR two PSG's. So I am an odd case! If the S9 doesn't work, hopefully some weightloss + continued aPAP will do the trick.
Anyone know the EM for the forum admin?
Anyone know the EM for the forum admin?