






I'm just trying to figure out what it means. Since you didn't ask that, can I assume you understand what it means and can shed some light on it?SleepingUgly wrote:NotMuffy wrote:Most important, have to figure out if the FLs were fixed or flow- or pressure-responsive (I mean, if the FLs were due to narrow nasal passages, it might be quite difficult to put a dent in them).
How do we figure that out?
.
Re: .
-
SleepingUgly

- Posts: 4690
- Joined: Sat Nov 28, 2009 9:32 pm
Re: .
I don't know exactly what it means, but I wanted to limit the number of questions I ask to increase the probability of getting them answered. But I assume it means that some anatomical structures may cause FLs that can't be altered by increasing the pressure. When I had my sleep study the doc said, "You had continuous FLs, and that's your nose". My anatomical issues were partly treated with surgery since then. I say partly because a septum can't be totally straightened in the back without doing cosmetic surgery and I didn't agree to nasal valve surgery. But I think anatomically my nose is fairly good, or at least better. However, congestion-wise I am not so good due to rhinitis that is incompletely treated. So if I still have FLs, is it due to fixed structures in my nose or does it respond to pressure increases? I think mine responds to pressure increases, but it's kinda hard to get good data because I can't wear the dang thing all night.LoQ wrote:I'm just trying to figure out what it means. Since you didn't ask that, can I assume you understand what it means and can shed some light on it?SleepingUgly wrote:NotMuffy wrote:Most important, have to figure out if the FLs were fixed or flow- or pressure-responsive (I mean, if the FLs were due to narrow nasal passages, it might be quite difficult to put a dent in them).
How do we figure that out?
I made all this up. I have no idea if it's right.
_________________
| Mask: Swift™ FX For Her Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Rescan 3.10 |
Never put your fate entirely in the hands of someone who cares less about it than you do. --Sleeping Ugly
Re: .
The part I was having trouble with was the "or flow- or" section.
The "fixed" made sense to me as an FL that, ironically, can't be fixed by changing the pressure because there are unyielding body parts or something.
The "pressure-responsive" made sense as an FL that would respond to pressure, and hence, more pressure might be helpful with that.
That leaves the "or flow- or". I guess the "or" things are conjunctions, heh.
The "fixed" made sense to me as an FL that, ironically, can't be fixed by changing the pressure because there are unyielding body parts or something.
The "pressure-responsive" made sense as an FL that would respond to pressure, and hence, more pressure might be helpful with that.
That leaves the "or flow- or". I guess the "or" things are conjunctions, heh.
-
SleepingUgly
- Posts: 4690
- Joined: Sat Nov 28, 2009 9:32 pm
Re: .
I assumed it meant "fixed or flow-responsive/pressure-responsive", although I'm not entirely sure what that means if they aren't synonyms. This is like the blind leading the blind.LoQ wrote:The part I was having trouble with was the "or flow- or" section.
The "fixed" made sense to me as an FL that, ironically, can't be fixed by changing the pressure because there are unyielding body parts or something.
The "pressure-responsive" made sense as an FL that would respond to pressure, and hence, more pressure might be helpful with that.
That leaves the "or flow- or". I guess the "or" things are conjunctions, heh.
_________________
| Mask: Swift™ FX For Her Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Rescan 3.10 |
Never put your fate entirely in the hands of someone who cares less about it than you do. --Sleeping Ugly
Re: .
Thank you Rebecca for asking, and thank you, MiniMuffy's grandad, for replying.
Something(s) I don't understand about the Flow Limitations:
If we think machines vary in reporting AHI for the same breathing pattern (of course we do) then I can attest from personal experience that reporting FL's is even less reliable: My GK420E showed me having tons of (that_company's_ defined) FL's, - the Respironics rarely any, the Resmed some. Rested Gal had the same PB / Respironics experience - other's too (on the forum) have reported that.
Now, assuming the GK420E (made by Puritan Bennett=PB) was driven skywards by nasal "hardware" - how come there was still some variability, and there's variablility in my FL's in on the Resmed - or in anyone elses?
In other words: why would we see variablitiy in a person's reported flow limitations (on any machine) if those flow limitations are caused by way the nose is built? Would this be a combination of how soft tissue varies during the night, and its interaction with the hard tissue?
Are you aware of any studies (or cases) showing positional FL' - could that happen theoretically?
O.
Something(s) I don't understand about the Flow Limitations:
If we think machines vary in reporting AHI for the same breathing pattern (of course we do) then I can attest from personal experience that reporting FL's is even less reliable: My GK420E showed me having tons of (that_company's_ defined) FL's, - the Respironics rarely any, the Resmed some. Rested Gal had the same PB / Respironics experience - other's too (on the forum) have reported that.
Now, assuming the GK420E (made by Puritan Bennett=PB) was driven skywards by nasal "hardware" - how come there was still some variability, and there's variablility in my FL's in on the Resmed - or in anyone elses?
In other words: why would we see variablitiy in a person's reported flow limitations (on any machine) if those flow limitations are caused by way the nose is built? Would this be a combination of how soft tissue varies during the night, and its interaction with the hard tissue?
Are you aware of any studies (or cases) showing positional FL' - could that happen theoretically?
O.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
-
SleepingUgly
- Posts: 4690
- Joined: Sat Nov 28, 2009 9:32 pm
Re: .
I don't know if this is what you mean, and certainly this is not a study... But the other night I decided to try to sleep on my back just to log some time without the mask leaking. I would doze and then wake feeling as if there was an influx of air, even though I was on straight CPAP and the pressure was constant. When I looked at the data the next day, I had sudden plummets from some degree of FLs to terrible FLs and then back up (I assume when I would wake). My flow limitations on my side were nothing compared to these.ozij wrote:Are you aware of any studies (or cases) showing positional FL' - could that happen theoretically?
I don't really know how to interpret just how bad my FLs are. I know when they are at the extremes, but I don't know how to interpret the rest. And of course I have no idea if they are associated with arousals. Muffy alluded to being able to infer when they are, so I'd like to hear more about that.
_________________
| Mask: Swift™ FX For Her Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Rescan 3.10 |
Never put your fate entirely in the hands of someone who cares less about it than you do. --Sleeping Ugly
Re: .
Me too.SleepingUgly wrote: Muffy alluded to being able to infer when they are, so I'd like to hear more about that.
And thanks for the info you added.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023

Re: .
In re: the company (AASM) line:
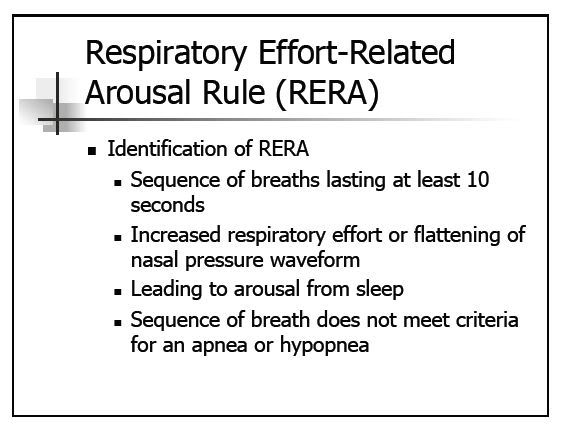
The new (although 3 years old already) rule states that the observation of "increased effort" is no longer mandatory, but having an arousal is. While arousals cannot technically be determined by waveform analysis, one might "infer" that one's there if there was some FL breathing terminated by a pile of recovery breaths.
However, a "spontaneous arousal" could create the same pattern (perhaps this was the point of Dr. Park's slide).
FL classically relates to diagnostic testing. Once you go on some sort of support, one has to take into account the performance of the machine. Most of the algorithms today tailor their waveforms to create "roundness" (like AFlex, or more dramatically, BiLevel therapy with it's IPAP fiddlement, optimizing rise times, the "Ocean Wave" of Malibu, etc.)
Anyway, this why BiLevel may be worth investigating in these cases. While pressure-responsive FL might simply respond to pressure increase (CPAP or EPAP), flow-responsive FL may (actually, by definition "would") respond to tailoring of the inspiratory waveform (IPAP, Rise-Time, or some sort of "comfort" technology).
But...
if one monitors neither effort nor arousals, one cannot tell if they are improving sleep quality (what you're really trying to do) or simply creating nice waveforms.
In other words, if one isn't creating additional negative intrathoracic pressure to get their breaths (but I don't know what the danger level is-- the Sleep reference says "loud" snorers), and the FLs do not generate arousals (as determined by NPSG, indirect inference, improved Epworth, or "I feel better"), then you're probably OK in leaving them alone.
And "IMHO", a huge percentage of patients who end up on sleep support forums (assuming they don't have a solid black bar on their Encore DLs) have "sleep" problems instead of "SDB" problems. This case was a great example, where sure, there were some excellent FLs to study, but if Sleep Efficiency is like 60%, it's the Yossarian metaphor (does anybody actually ever pay attention to anything except "Techno-Flash"!??)("Wow, let's take apart ResScan and make the background fuschia!"}{Whoops! Sorry! That was me!)
The new (although 3 years old already) rule states that the observation of "increased effort" is no longer mandatory, but having an arousal is. While arousals cannot technically be determined by waveform analysis, one might "infer" that one's there if there was some FL breathing terminated by a pile of recovery breaths.
However, a "spontaneous arousal" could create the same pattern (perhaps this was the point of Dr. Park's slide).
FL classically relates to diagnostic testing. Once you go on some sort of support, one has to take into account the performance of the machine. Most of the algorithms today tailor their waveforms to create "roundness" (like AFlex, or more dramatically, BiLevel therapy with it's IPAP fiddlement, optimizing rise times, the "Ocean Wave" of Malibu, etc.)
Anyway, this why BiLevel may be worth investigating in these cases. While pressure-responsive FL might simply respond to pressure increase (CPAP or EPAP), flow-responsive FL may (actually, by definition "would") respond to tailoring of the inspiratory waveform (IPAP, Rise-Time, or some sort of "comfort" technology).
But...
if one monitors neither effort nor arousals, one cannot tell if they are improving sleep quality (what you're really trying to do) or simply creating nice waveforms.
In other words, if one isn't creating additional negative intrathoracic pressure to get their breaths (but I don't know what the danger level is-- the Sleep reference says "loud" snorers), and the FLs do not generate arousals (as determined by NPSG, indirect inference, improved Epworth, or "I feel better"), then you're probably OK in leaving them alone.
And "IMHO", a huge percentage of patients who end up on sleep support forums (assuming they don't have a solid black bar on their Encore DLs) have "sleep" problems instead of "SDB" problems. This case was a great example, where sure, there were some excellent FLs to study, but if Sleep Efficiency is like 60%, it's the Yossarian metaphor (does anybody actually ever pay attention to anything except "Techno-Flash"!??)("Wow, let's take apart ResScan and make the background fuschia!"}{Whoops! Sorry! That was me!)
"Don't Blame Me...You Took the Red Pill..."
-
NightMonkey

- Posts: 801
- Joined: Sat Jan 15, 2011 2:43 pm
- Location: Three seats, orchestra right
Re: .
That must have taken a lot of effort to delete 500 posts.
What happened to Secret Agent Girl?
What happened to Secret Agent Girl?
NightMonkey
Blow my oropharynx!
the hairy, hairy gent who ran amok in Kent
Blow my oropharynx!
the hairy, hairy gent who ran amok in Kent
Re: .
No one on the planet sleeps perfectly, and no one on the planet breathes perfectly. But if someone doesn't feel well, he may feel better with some airway pressure, if that improves his sleep. The rest is details.
In the context of sleep medicine, all the different names for all the varieties of the imperfections of breathing are only labels used to prove to the money people that a person's breathing is imperfect during sleep. (Which, scientifically speaking, is a pretty silly thing to prove, since everyone knows it is true of everyone.)Then the re-measurements "prove" something supposedly got "treated" in that it can't be measured anymore.
The bottom line is that if a doc sees indications that a person should try PAP, the numbers can easily get massaged and the labels moved around to make sure that treatment gets paid for. The problem with that is that sometimes the money people figure that out and push back and say: "Hey, wait a minute fellas--you can't use that particular measurement to make us pay for things." Then the docs have to find a way around that limitation by measuring something else and using that as "proof" to the money people.
After all, the most important form of flow limitation in the sleep industry is anything that limits the flow of money for treating patients. We as patients can't let that little game throw us off too much.
If there are indications that a patient might benefit from trying PAP, a doc is likely to point to any blip on a squiggly and say: "There it is! I'm treating THAT!" It doesn't matter to the doc whether the "that" is a heart oscillation, artifact, sun-spot activity, earth-rotation wobble, wayward neutrinos, or bubbles in the time-space continuum. All he really cares about is patient response to therapy. Why it works doesn't really matter to him, but he has to pretend it does in order to keep the money people happy.
The various machines are just tools that deliver the pressure differently, and some patients respond better to one kind of machine than to another. The money people want docs to try the cheapest machine first. If bilevel was cheaper than CPAP, everyone would be prescribed bilevel first and would have to "fail" it to qualify for CPAP. If the ASVs were cheaper, everyone would have to start out on that. The only PAP choices in front of a doc are amount of pressure and type of machine. Other than that, we start moving into drugs designed more for treating symptoms than causes.
Docs are about trying things to see if patients feel better. Take drugs, for example. Docs don't understand all the details of why a particular drug helps patients, or which blip on a squiggly is being obscured, but they prescribe the drugs anyway and realize that every human is different in his response to every drug. The doc just says: "Try taking an aspirin and see if the headache goes away." If that doesn't help, there are other things to try. Since insurance isn't involved, a lot of tests and measurements don't come into play, since the testing would be more expensive than the treatments tried.
Funny thing is, sleep medicine finds itself in the awkward position of its testing costing much more than simply trying the treatment, too. And renaming squiggly blips won't change that. Once the money people completely figure that out, all heck is gonna break loose.
In my opinion.
But I could be as wrong about all that as I could be about why the agent went into deep cover.
In the context of sleep medicine, all the different names for all the varieties of the imperfections of breathing are only labels used to prove to the money people that a person's breathing is imperfect during sleep. (Which, scientifically speaking, is a pretty silly thing to prove, since everyone knows it is true of everyone.)Then the re-measurements "prove" something supposedly got "treated" in that it can't be measured anymore.
The bottom line is that if a doc sees indications that a person should try PAP, the numbers can easily get massaged and the labels moved around to make sure that treatment gets paid for. The problem with that is that sometimes the money people figure that out and push back and say: "Hey, wait a minute fellas--you can't use that particular measurement to make us pay for things." Then the docs have to find a way around that limitation by measuring something else and using that as "proof" to the money people.
After all, the most important form of flow limitation in the sleep industry is anything that limits the flow of money for treating patients. We as patients can't let that little game throw us off too much.
If there are indications that a patient might benefit from trying PAP, a doc is likely to point to any blip on a squiggly and say: "There it is! I'm treating THAT!" It doesn't matter to the doc whether the "that" is a heart oscillation, artifact, sun-spot activity, earth-rotation wobble, wayward neutrinos, or bubbles in the time-space continuum. All he really cares about is patient response to therapy. Why it works doesn't really matter to him, but he has to pretend it does in order to keep the money people happy.
The various machines are just tools that deliver the pressure differently, and some patients respond better to one kind of machine than to another. The money people want docs to try the cheapest machine first. If bilevel was cheaper than CPAP, everyone would be prescribed bilevel first and would have to "fail" it to qualify for CPAP. If the ASVs were cheaper, everyone would have to start out on that. The only PAP choices in front of a doc are amount of pressure and type of machine. Other than that, we start moving into drugs designed more for treating symptoms than causes.
Docs are about trying things to see if patients feel better. Take drugs, for example. Docs don't understand all the details of why a particular drug helps patients, or which blip on a squiggly is being obscured, but they prescribe the drugs anyway and realize that every human is different in his response to every drug. The doc just says: "Try taking an aspirin and see if the headache goes away." If that doesn't help, there are other things to try. Since insurance isn't involved, a lot of tests and measurements don't come into play, since the testing would be more expensive than the treatments tried.
Funny thing is, sleep medicine finds itself in the awkward position of its testing costing much more than simply trying the treatment, too. And renaming squiggly blips won't change that. Once the money people completely figure that out, all heck is gonna break loose.
In my opinion.
But I could be as wrong about all that as I could be about why the agent went into deep cover.
Last edited by jnk on Thu Feb 10, 2011 8:02 am, edited 1 time in total.

Re: .
Mini-Muffy is adorable. Congratulations!
Thanks for all the info you're giving us.
I'm all for Techno-flash, but please, please don't turn the background fuchsia, it hurts my eyes and makes me cranky.
r
Thanks for all the info you're giving us.
Sorry to make this so remedial, but do you have a picture/graphic of what recovery breaths look like? If I had to guess, I would guess that they show up as a pile of taller and skinnier waveforms (is that the right word?) in the flow.NotMuffy wrote:
The new (although 3 years old already) rule states that the observation of "increased effort" is no longer mandatory, but having an arousal is. While arousals cannot technically be determined by waveform analysis, one might "infer" that one's there if there was some FL breathing terminated by a pile of recovery breaths.
Spontaneous arousals are evil. They distort everything. I have been inferring that I am having more spontaneous arousals when there are more centrals in my data.However, a "spontaneous arousal" could create the same pattern (perhaps this was the point of Dr. Park's slide).
So then in the unlikely case that the settings were incorrect, it is possible to go back and confirm whether or not the arousals are spontaneous or FL related.NotMuffy wrote: As long as the hardware filters are set correctly, software filter-wingin' can occur any time, as much as you want, either during collection or analysis.
I would guess an even bigger catch-22 for people with SDB problems combined with sleep problems.And "IMHO", a huge percentage of patients who end up on sleep support forums (assuming they don't have a solid black bar on their Encore DLs) have "sleep" problems instead of "SDB" problems. This case was a great example, where sure, there were some excellent FLs to study, but if Sleep Efficiency is like 60%, it's the Yossarian metaphor (does anybody actually ever pay attention to anything except "Techno-Flash"!??)("Wow, let's take apart ResScan and make the background fuschia!"}{Whoops! Sorry! That was me!)
I'm all for Techno-flash, but please, please don't turn the background fuchsia, it hurts my eyes and makes me cranky.
r
-
SleepingUgly
- Posts: 4690
- Joined: Sat Nov 28, 2009 9:32 pm
Re: .
NotMuffy wrote:In re: the company (AASM) line:
The new (although 3 years old already) rule states that the observation of "increased effort" is no longer mandatory, but having an arousal is.
Is flattening of the nasal pressure waveform = FL? If so, is that still an integral part of the criteria?
So EPR turned on tends to help the FLs as opposed to CPAP or APAP with EPR off?FL classically relates to diagnostic testing. Once you go on some sort of support, one has to take into account the performance of the machine. Most of the algorithms today tailor their waveforms to create "roundness" (like AFlex, or more dramatically, BiLevel therapy with it's IPAP fiddlement, optimizing rise times, the "Ocean Wave" of Malibu, etc.)
Anyway, this why BiLevel may be worth investigating in these cases.
Cases where the person appears to have FLs on CPAP and continued EDS?
OK, so is there a way to tell from CPAP data whether it's a pressure-responsive or flow-responsive FL? (and are those mutually exclusive or can a person have both?)While pressure-responsive FL might simply respond to pressure increase (CPAP or EPAP), flow-responsive FL may (actually, by definition "would") respond to tailoring of the inspiratory waveform (IPAP, Rise-Time, or some sort of "comfort" technology).
Meaning that in those cases, the residual FLs are not likely to be the cause of the EDS?In other words, if one isn't creating additional negative intrathoracic pressure to get their breaths (but I don't know what the danger level is-- the Sleep reference says "loud" snorers), and the FLs do not generate arousals (as determined by NPSG, indirect inference, improved Epworth, or "I feel better"), then you're probably OK in leaving them alone.
And short of the person being aware of poor sleep efficiency, how do we know if there's a sleep problem vs. an SDB problem? For example, I wake up several times a night, but I tend to go back to sleep quickly. Given that the number of "spontaneous arousals" my sleep studies always reported were tons more than the number of times I remember waking up (which is still too many times compared to "normals"), I always assumed that for every time I remember waking, I probably have many more "arousals" that are too brief for me to remember.And "IMHO", a huge percentage of patients who end up on sleep support forums (assuming they don't have a solid black bar on their Encore DLs) have "sleep" problems instead of "SDB" problems.
Thank you so much for not dropping this thread, and us, and for continuing to help!
_________________
| Mask: Swift™ FX For Her Nasal Pillow CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Rescan 3.10 |
Never put your fate entirely in the hands of someone who cares less about it than you do. --Sleeping Ugly