mdboze wrote:Thank you:
JohnBFisher,
Banned,
dsm,
for your feedback regarding the PS settings on my PiPap autoSV Advanced.
Rather than just make the PS change myself, I called my DME who set it up the unit to confirm the correct settings, they will call me back tomorrow.
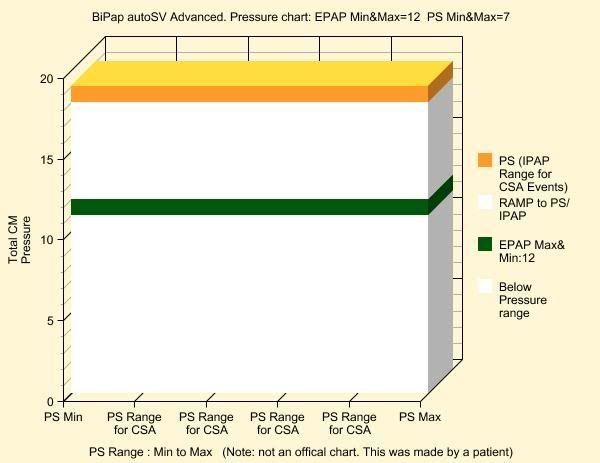
Since I know they set EPAP min=12 ; EPAP max=7 (which was backwards) whch caused both min and max setttings got set to 12.
I'm 95% sure they also got the PS settings backwards and set PS min=20 and PS max=7, which caused both PS max and min to get set to 7.
But to be sure.... I'll wait for their call tomorrow.
Hmm-mmm...
If the DME found out that I know how to get into the setup mode; I bet they will think I changed it, and not take ownership of the screwup.
Anyone known if accessing the setup is logged on the smartcard ?
mdboze
I don't believe so - the card can be used to change the settings but it doesn't create an activity log of what you do on the machine other than the internal data does show what settings were on each day.
The way the EpapMin & EpapMax work from what I understand after looking at the titration guide (this is only my interpretation) ...
A:
EpapMin = starting Epap Pressure & thus the base pressure off which other pressures happen
EpapMax = the pressure the machine will go up to if OSA events are detected and dealt with
B:
PSMin = gets added to epap. Thus, sets the gap between epap & ipap (in this case, epap is what ever pressure the machine is currently at allowing A: above)
PSMax = gets added to the current epap to determine the max pressure that the SV support will ramp up to if SV events are being responded to. SV will only work if PSMax is greater than PSMin.
Assuming the above is correct then it probably means the following will happen ...
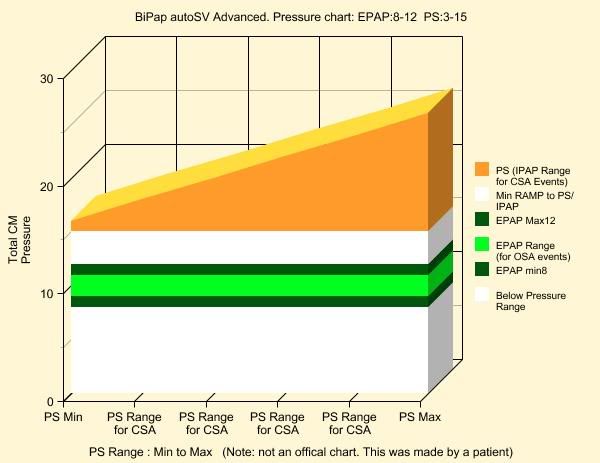
If EpapMin were set to say 8 CMs & EpapMax were set to say 12 CMs then the machine has a 4 CMs range to adjust epap if it detects snoring & obstructive (close airway) apneas.
If PSMin were set to say 3, then when epap=8, ipap would be at 8+3 but as epap gets raised by detected OSA events ipap would also rise with epap. Thus if after 4 hrs sleep the machine had raised epap to 10 CMs in response to OSA events, then ipap would be running at 13 CMs at that time. If EpapMax (12) got reached then ipap would nominally be at 15 CMs.
If PSMax is set to the same value (or less) than PSMin then SV support is not active.
If PSMax is set to a value above PSMin, then SV is activated & if PB or CA (open airway apnea) or other monitored activity is detected the SV algorithm will kick in. SV while doing its support will stop when it reaches PSMax above current (instantaneous) epap pressure.
So if we set PSMin to say 3 and PSMax to say 15, then at the start of the night we would see ...
epap=8 - ipap=11
epap auto titration would have the potential to increase epap from 8 to 12 as required, if osa gets detected & epap gets raised, both epap & ipap will be increased by the same pressure value as already indicated.
SV would be able to add up to 15 CMs above what ever the current epap was at the moment SV got activated.
SV attempts to bring the user back to target (normalize) av peak flow within 3 breathing cycles.
DSM