NotMuffy wrote:
However, there's also a lot of stable Duece in there as well......
so when you have stable sleep, you have stable breathing.
Yeah, and? No smoke and mirrors with that statement. Not sure what you're getting at......
Are you basically saying the increase in AHI is simply due to post-arousal hypopventilation, due to increased arousability as a result of compressing the abdomen and has nothing to do with changing the mechanics of the upper airway? How can I prove that the increased arousals weren't simply due to respiratory events OR due to making it harder for them to sleep? What's causing what?
NotMuffy wrote:Yes we used magnetometers to measure changes in FRC with compression. We measured A-P and lateral dimensions of the chest and abdomen. I haven't analyzed this data yet and it's going to take a bit of work. In a perfect world, we would have liked to measure absolute FRC. This is in the "too hard basket" as this stage unless we get patients to sleep in a body box.
I meant doing it while awake.
No we didn't measure changes during wakefulness. We were more concerned with what happened during sleep.
NotMuffy wrote:
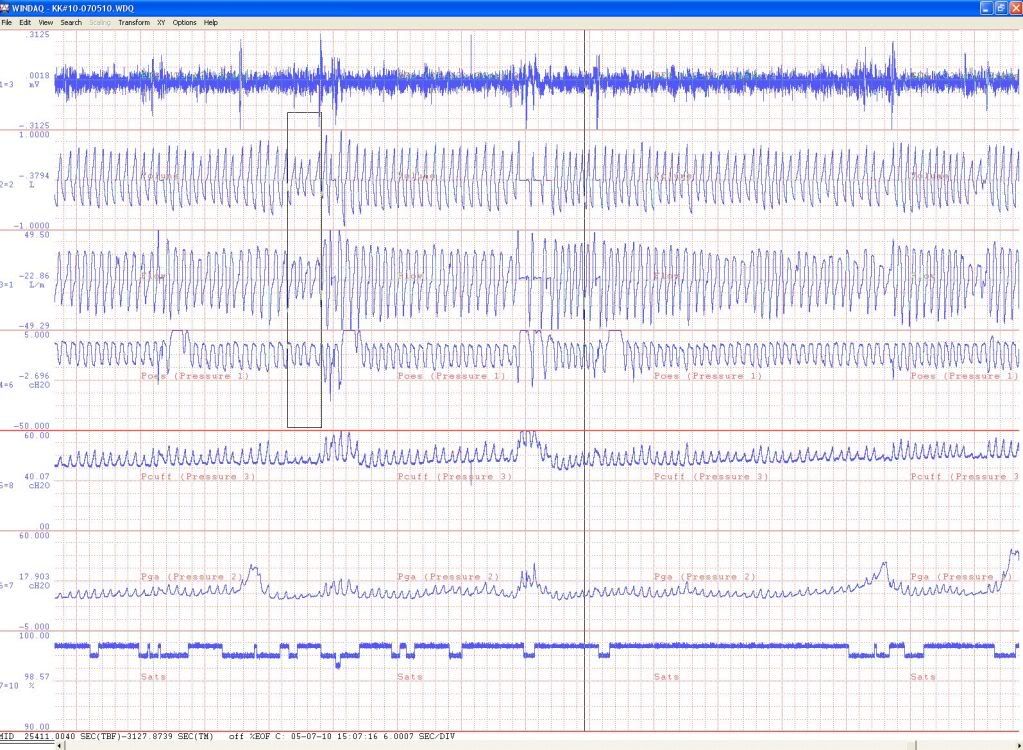
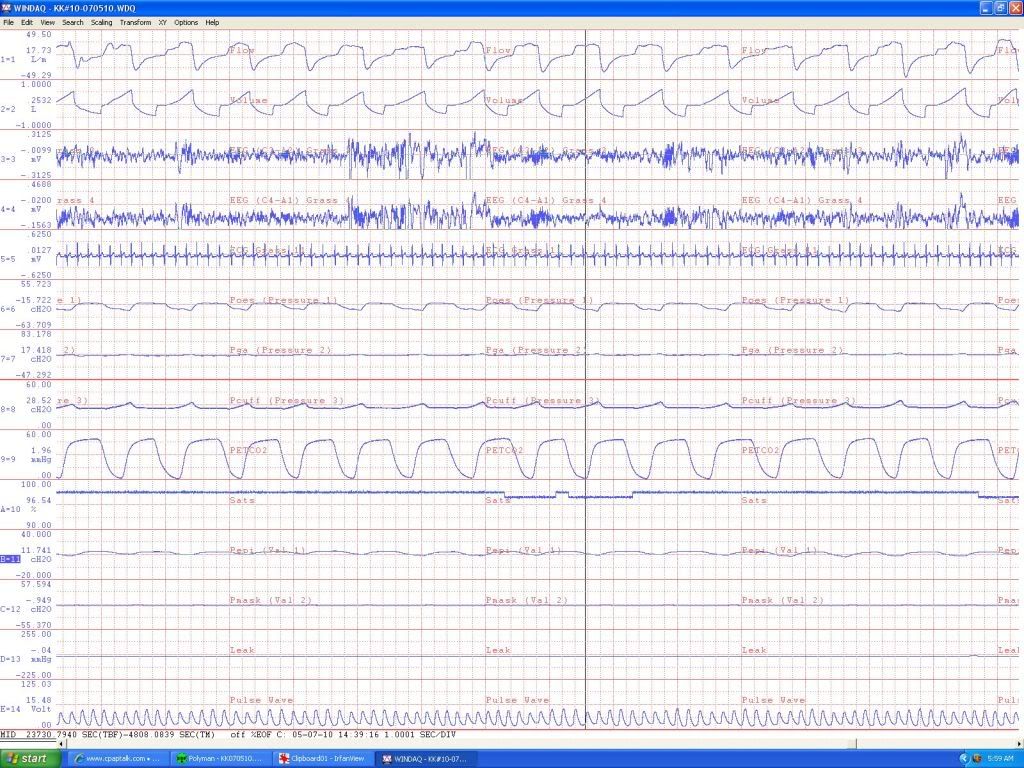
Yes, I did see that, but I think you gotta get your babe to incorporate that Pes in scoring and cull out those central hypopneas, cause there were a lot.
If that's the case, why shouldn't we measure Pes in all PSGs?
I think that's being a bit harsh to exclude them all. Now without looking at any PSGs, I would predict a number of hypopneas, that directly follow arousals, would start as one of these central hypopneas i.e. period of hypoventilation and decrease in Pes swing as drive dissipates after the initial period of post-arousal hyperventilation. As the hypopnea continues, drive would likely increase (greater swings in Pes) due to mechano- and chemo- stimuli. Do I exclude these events as well? Do I exclude any events which don't show at least 1 breath of increased drive? Or do I exclude any events which occur directly after an arousal? At the end of the day, these are still respiratory events.
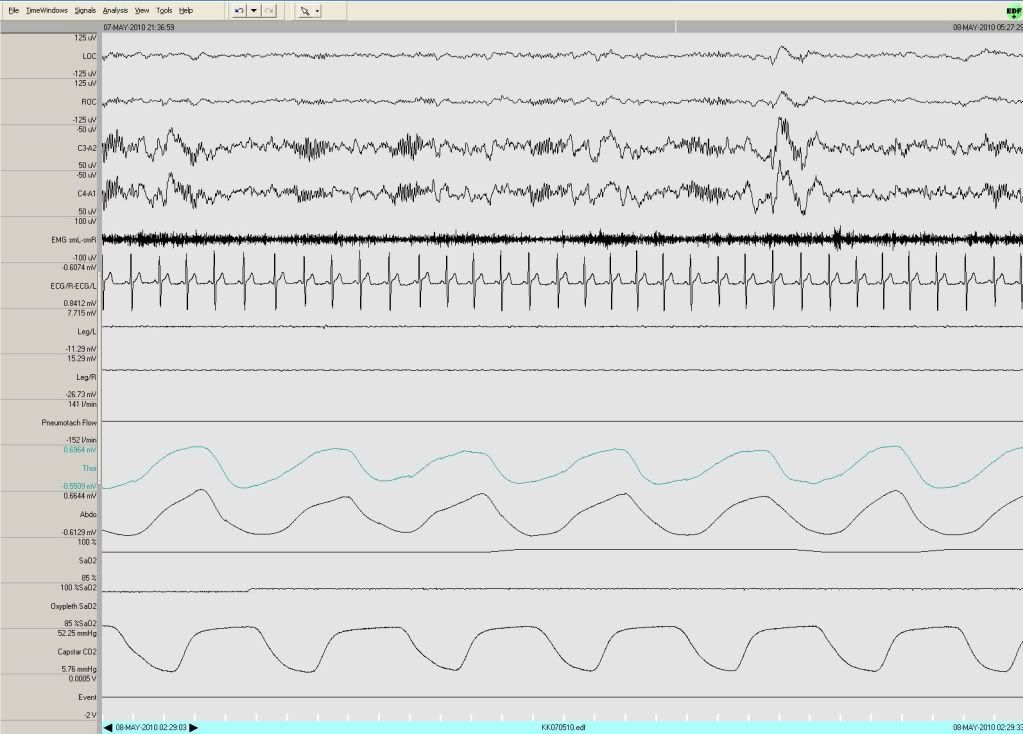
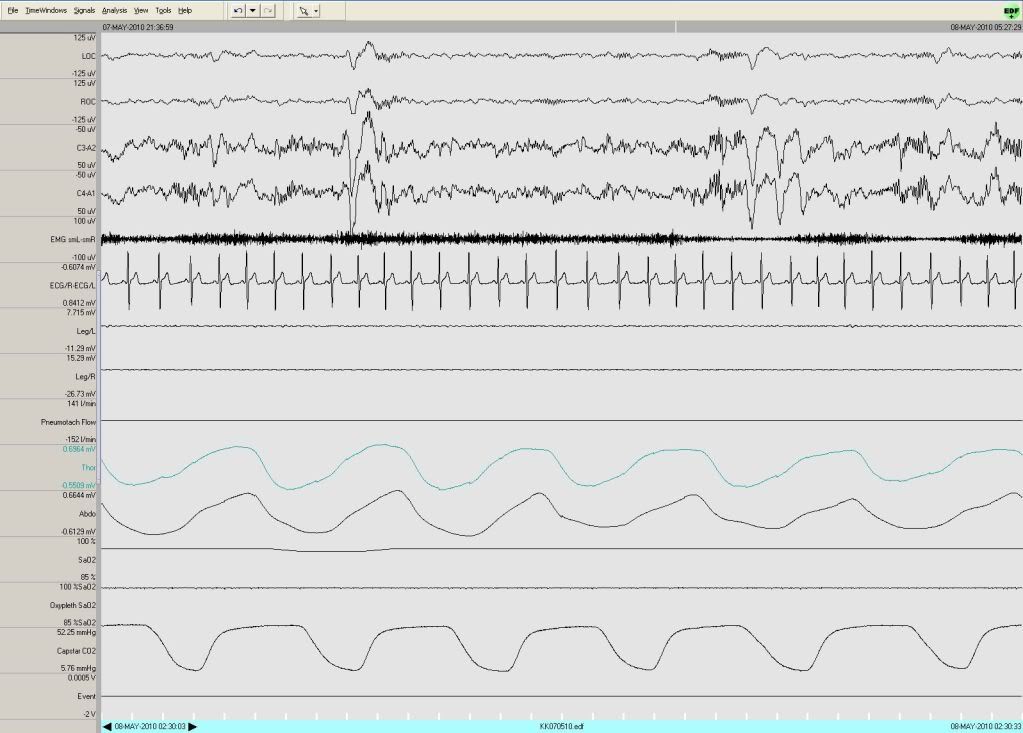
NotMuffy wrote:Also, can you get this guy's drug list (if any, legal or not)(assuming you guys got laws over there). He seems to be putting up a lot of spindles.
Will need to check when I get to work. Can't recall him being on any drugs though.