








I recently joined and posted an intro in this thread. I am not a healthcare professional and am not an expert on sleep, but I work in neuroscience and physiology research and have access to monitoring equipment. I’m waiting for results from an overnight test I did last week with a sleep clinic, but in the meantime I have been having some ‘fun’ monitoring my expired O2 and CO2 during the night.
The observations are intriguing (to me at least), and I would be very interested if anyone who has more expertise could comment. Basically I have long periods of normal breathing, with clusters of the regular apneas as shown in the graphs below:
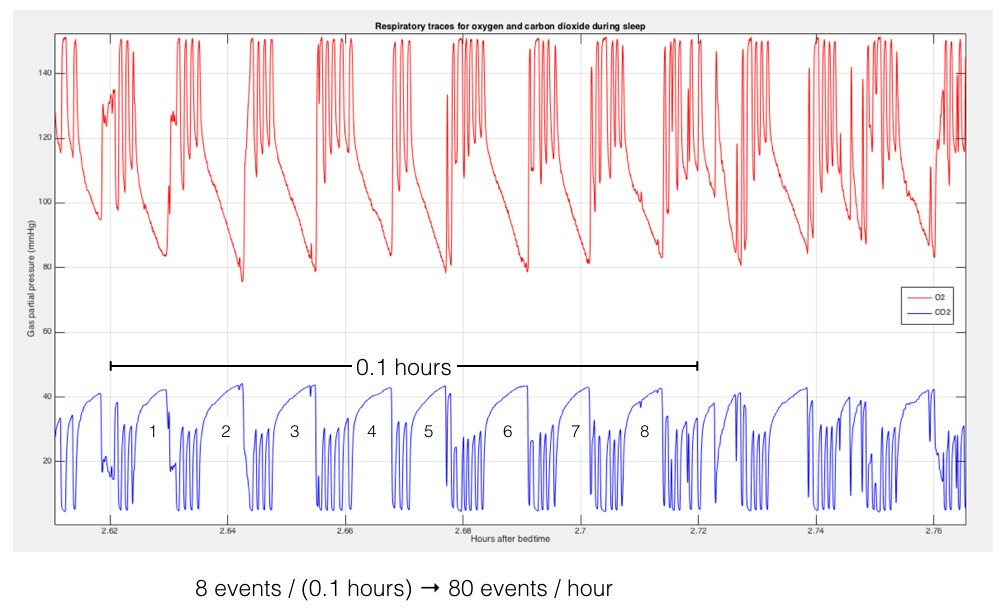
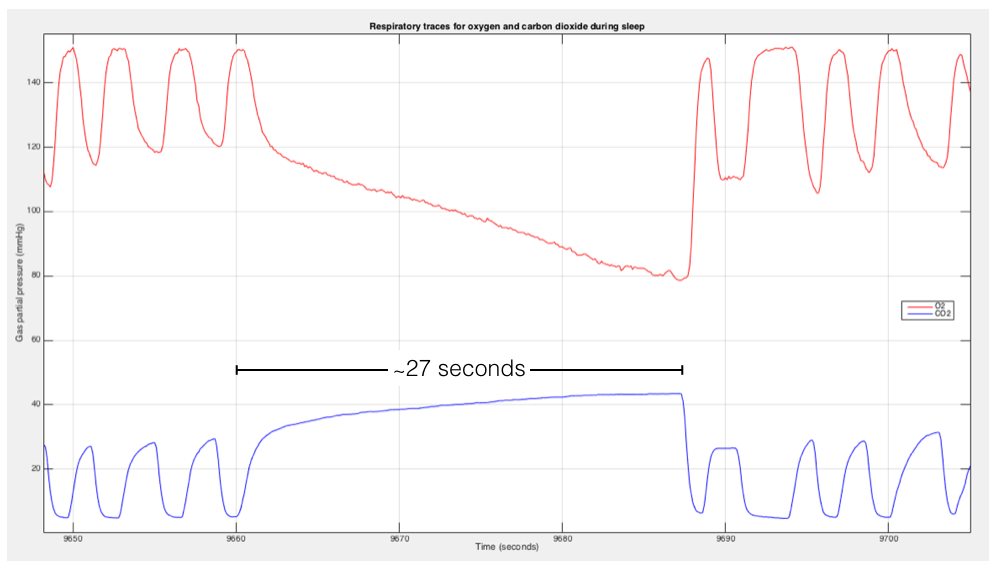
Please note that, although the ‘rate’ of apneas during these clusters corresponds to around 80/hour, the clusters don’t actually last an hour so my AHI is probably nowhere near 80. The graph below zooms in to show several regular breaths followed by an apnea lasting around 27 seconds. Please also note that the O2 value shown here is *not* saturation, but rather the level of O2 in exhaled air (which is related to O2 sat but not the same thing). It's only a coincidence that the O2 partial pressure drops to 80mmHg - that's not the same thing as an O2 sat of 80%, although it is abnormally low.
The timing of the clusters looks suspiciously like they arise when REM sleep would normally occur; as I noted in my other post I had a sleep study years ago that indicated narcolepsy, in part because I entered REM sleep very rapidly after turning out the lights (and in part because I entered REM rapidly and repeatedly during daytime sleep tests the next day). That test was done when I was young and thin , and did not indicate any sleep apnea issues.
This image shows the general timing of the apnea clusters:

This one shows an interval of normal breathing:

(*note: the fact that the CO2 trace does not go down to zero indicates there is a small amount of rebreathing from dead space in my improvised mask; the setup is normally used with medical air blowing in through one-way valves but I wasn’t going to drag an h-size cylinder home. I modified the mask some to minimize dead space, but would probably use a mouthpiece to do this for real. Should not affect breathing rate or values significantly.)
I am wondering if anyone can comment on whether clusters of apnea like this are typical, and (while I wait for my doc’s report), what the significance might be.





