






Me smacking my forehead. "!" I should have remembered the first thing to check is whether or not some graphs are simply omitted from the graphs section. Simple solution.Papit wrote: -Nate and DreamDiver, you put me on the right track with your comments and questions. I can now bring up both Flow and Flow Limitation in the Detailed Graphs.
0.0
-
DreamDiver

- Posts: 3082
- Joined: Thu Oct 04, 2007 11:19 am
Re: 0.0
_________________
| Mask: ResMed AirFit™ F20 Mask with Headgear + 2 Replacement Cushions |
| Additional Comments: Pressure: APAP 10.4 | 11.8 | Also Quattro FX FF, Simplus FF |

Re: 0.0
-Nate and DreamDiver, you put me on the right track with your comments and questions. I can now bring up both Flow and Flow Limitation in the Detailed Graphs. Check it out and see the way I did it below the image. I think all S9 VPAP Adapt users (maybe all S9 users) can do the same to view Flow and Flow Limitation and/or other graphs. ResMed isn't hiding the charts. It's more a matter of navigation and selecting what you want (and don't want) to see.NateS wrote:Would these be relevant or helpful?: (earlier links)DreamDiver wrote:Curious indeed. Fantastic! Thanks. I'm learning a lot. I'd never have guessed that ResMed would hide flow on the ASV, and I'm not sure why they would. . . .Papit wrote:... Note that I had to use SH to see the Flow Rate graph. Although I see "Flow" (in addition to "Flow Limitation" and the usual graphs) listed under Tools>Options>Preferences>Detailed Graphs>Graphs, no "Flow" graph comes up for me except "Flow Limitation". Curious.idamtnboy wrote: 10/26/2011
Regards, Nate

Select a date within the last couple days; then go into the Report menu and create a report. Select Customize, then expand 'Detailed Graphs' in the right-hand column. Expand 'Detailed Graphs' again under Available Items on the left. Now select Flow Limitation and Flow from the left if you don't have and want to add either or both graphs and then 'Add' them to your current list of graphs. If you want to get rid of any current detailed graphs that you don't want (clutter), 'Remove' them from your list on the right. You can always go back when you want to reconfigure your list. This is also a good opportunity to resequence the order in which the graphs are displayed to you. When done, click OK and do a File>Save.
Best regards. Thanks again for working on this with me.
_________________
| Mask: DreamWear Nasal CPAP Mask with Headgear |
| Additional Comments: Machine: AirCurve 10 ASV (37043), Software:ResScan 5.7.0.9477, SleepyHead V1.00BETA2, Oximeter:CMS-50i |
Machine: AirCurve 10 ASV, Mask: AirFit N30i
PulseOx Data-transfer to OSCAR4-23-12http://tinyurl.com/nzd64gu
Wireless SD Card Data-transfer to OSCAR 8-14-15http://tiny.cc/z1kv8x
PulseOx Data-transfer to OSCAR4-23-12http://tinyurl.com/nzd64gu
Wireless SD Card Data-transfer to OSCAR 8-14-15http://tiny.cc/z1kv8x
-
DreamDiver
- Posts: 3082
- Joined: Thu Oct 04, 2007 11:19 am
Re: 0.0
Thanks NateNateS wrote:Would these be relevant or helpful?:
...
viewtopic.php?f=1&t=70181&p=649833&hili ... ml#p649833
and:
Editing the ResScan XML Files to Show Me What I want
viewtopic.php?f=1&t=64986&p=606916&hili ... ml#p606916
...
_________________
| Mask: ResMed AirFit™ F20 Mask with Headgear + 2 Replacement Cushions |
| Additional Comments: Pressure: APAP 10.4 | 11.8 | Also Quattro FX FF, Simplus FF |

Re: 0.0
Would these be relevant or helpful?:DreamDiver wrote:Curious indeed. Fantastic! Thanks. I'm learning a lot. I'd never have guessed that ResMed would hide flow on the ASV, and I'm not sure why they would. There is probably a file edit for that to make it show on ResScan, if you want to. I'm guessing one of the other forum members will figure it out before I do, if it hasn't been figured out already, but since the data exist, it should be too difficult to make ResScan see your flow data on the ASV.Papit wrote:... Note that I had to use SH to see the Flow Rate graph. Although I see "Flow" (in addition to "Flow Limitation" and the usual graphs) listed under Tools>Options>Preferences>Detailed Graphs>Graphs, no "Flow" graph comes up for me except "Flow Limitation". Curious.
I don't know enough to make suggestions about pressure changes, but I'm interested in following along on to hear how things progress. Again, thanks.
viewtopic.php?f=1&t=70181&p=649833&hili ... ml#p649833idamtnboy wrote: 10/26/2011
OK, I just happened to remember. You have to make some edits to the resscan.xml file in order to get Resscan to display it. Search flow limitation and xml. You should be able to find the thread where it's discussed.
and:
Editing the ResScan XML Files to Show Me What I want
viewtopic.php?f=1&t=64986&p=606916&hili ... ml#p606916
Regards, Nate
_________________
| Mask: DreamWear Nasal CPAP Mask with Headgear |
| Additional Comments: ResMed AirCurve 10 ASV; Dreamwear Nasal Mask Original; CPAPMax Pillow; ResScan & SleepyHead |
Central sleep apnea AHI 62.6 pre-VPAP. Now 0 to 1.3
Present Rx: EPAP: 8; IPAPlo:11; IPAPHi: 23; PSMin: 3; PSMax: 15
"I've had a perfectly wonderful evening, but this wasn't it." —Groucho Marx
Present Rx: EPAP: 8; IPAPlo:11; IPAPHi: 23; PSMin: 3; PSMax: 15
"I've had a perfectly wonderful evening, but this wasn't it." —Groucho Marx
-
DreamDiver
- Posts: 3082
- Joined: Thu Oct 04, 2007 11:19 am
Re: 0.0
Curious indeed. Fantastic! Thanks. I'm learning a lot. I'd never have guessed that ResMed would hide flow on the ASV, and I'm not sure why they would. There is probably a file edit for that to make it show on ResScan, if you want to. I'm guessing one of the other forum members will figure it out before I do, if it hasn't been figured out already, but since the data exist, it should not be too difficult to make ResScan see your flow data on the ASV.Papit wrote:... Note that I had to use SH to see the Flow Rate graph. Although I see "Flow" (in addition to "Flow Limitation" and the usual graphs) listed under Tools>Options>Preferences>Detailed Graphs>Graphs, no "Flow" graph comes up for me except "Flow Limitation". Curious.
I don't know enough to make suggestions about pressure changes, but I'm interested in following along on to hear how things progress. Again, thanks.
_________________
| Mask: ResMed AirFit™ F20 Mask with Headgear + 2 Replacement Cushions |
| Additional Comments: Pressure: APAP 10.4 | 11.8 | Also Quattro FX FF, Simplus FF |
Last edited by DreamDiver on Sun Jun 30, 2013 7:52 pm, edited 1 time in total.

Re: 0.0
Are we going to deal now with Papit's Flow Limitation?



Check this about Flow Limitation (consisting of RERAs and UARs):
A source for a link:
http://www.apneaboard.com/forums/Thread ... e-Syndrome
Do you have Upper Airway Resistance Syndrome (UARS)?
Clinical Features
Patients with UARS have symptoms similar to those seen in OSAS, although there are some distinct features. Much of the research performed has attempted to identify and describe a group of patients with significant daytime sleepiness and disrupted sleep, but without the other dominant clinical features seen in OSAS. Typical symptoms reported by patients with UARS include excessive daytime sleepiness, fatigue, difficulty concentrating, morning headaches, and unrefreshing sleep. There can be also be a significant impairment in daytime functioning; a recent study demonstrated that subjects with UARS performed worse than patients with obstructive sleep apnea hypopnea syndrome and normal control individuals on different aspects of the Psychomotor Vigilance Task. In a separate study, upwards of 30% of subjects with UARS had abnormal sleep-onset latency on the Maintenance of Wakefulness Test. Individuals with abnormal airway anatomy are at increased risk, including those with a decreased retrolingual space, narrow nasal passages, or a small neck circumference. Patients are typically not obese, with a mean BMI often <25 kg/m. They are also usually younger than those in whom OSAS is diagnosed, with a mean age of approximately 38 years. Snoring is not a requisite symptom, with 10% to 15% or more of patients having never or only intermittently snored.
Patients with UARS are also more likely to report symptoms of frequent nocturnal awakening with difficulty falling back to sleep. This is thought to be a potential reason for increased complaints of insomnia amongst patients with UARS, including sleep onset and sleep maintenance problems. In addition to difficulties with acute insomnia, patients with UARS also have an increased likelihood of carrying a diagnosis of chronic insomnia. Other notable complaints include parasomnias, especially sleepwalking, sleep talking, and sleep terrors. Patients may also have symptoms of abnormal autonomic function, including lightheadedness or dizziness on rising from a supine or sitting position, cold hands and feet, and low resting blood pressures (defined as a systolic BP <105 mm Hg with a diastolic BP <65 mm Hg). In a study of 400 patients with UARS, more than 20% met criteria for low BP, a significantly higher prevalence when compared with people who have OSAS (0.6%) or insomnia (0.9%). Interestingly, all subjects in the study had evidence of a small oral cavity on examination with a narrowed airway space dimension on cephalometric radiographs, consistent with other reports. Lastly, patients with UARS have increased rates of symptoms such as gastroesophageal reflux, muscular pain, diarrhea, abdominal pain, depression, and anxiety. This has led some authors to suggest a link between UARS and functional somatic syndromes, such as irritable bowel syndrome, chronic fatigue syndrome, and fibromyalgia. In a study of 75 subjects equally divided into three groups (UARS, mild to moderate OSAS, and severe OSAS), those with UARS were more likely to report symptoms of headache, irritable bowel symptoms, and sleep-initiation insomnia. Subjects with UARS were also more likely to have alpha intrusion during slow-wave sleep, a polysomnographic finding described in a number of fatigue syndromes. In children with UARS, symptoms consistent with attention deficit disorder or attention deficit hyperactivity disorder may be present, with behavioral changes leading to poor school performance.
________________________________________
Clinical Features Associated With UARS
Daytime symptoms:
Excessive daytime sleepiness
Fatigue
Morning headaches
Myalgia’s [muscle pain]
Difficulty concentrating
Sleep disturbances:
Frequent nocturnal awakenings
Difficulties initiating sleep
Insomnia
Bruxism [teeth clenching]
Restless leg syndrome
Unrefreshing sleep
Autonomic nervous system:
Hypotension
Orthostasis [maintenance of an upright standing posture]
Cold hands and feet
Functional somatic syndrome associations:
Depression
Anxiety
Chronic fatigue syndrome
Irritable bowel syndrome
Fibromyalgia
Polysomnographic abnormalities Increased RERAs:
Increased nocturnal arousals
Increased CAP rate [cyclical alternating pattern in EEG]
Alpha intrusion during sleep
Treatment
The optimal treatment for patients with UARS is not currently known. Continuous positive airway pressure (CPAP) has been quite useful in the treatment of sleep-disordered breathing and there are some notable positive results in CPAP treatment of UARS. In a study of 15 heavy snorers with clinical evidence of UARS, treatment with nasal CPAP was associated with decreases in observed nocturnal arousals on polysomnography and decreases in mean sleep latency times on multiple sleep latency testing (MSLT) after several nights of treatment. A follow-up study of 15 subjects (in the original description of UARS) with daytime sleepiness and fatigue and who had undergone a therapeutic trial of positive pressure therapy reported similar findings. After treatment with approximately a month of nasal CPAP, significant improvements were seen in mean sleep latency times on MSLT (5.3 minutes vs 13.5 minutes), Pes nadir pressure (–33.1 cm H2O vs –5.3 cm H2O), amount of slow-wave sleep (1.2% vs 9.7%), and EEG arousals (31.3 vs 7.9 events/hour of sleep). Along with an improvement in sleep latency times on MSLT, there were subjective reports of improved daytime symptoms. Lastly, in a study of 130 postmenopausal women with chronic insomnia and evidence of UARS (n=62) or normal breathing (n=68), treatment with either nasal turbinectomy or nasal CPAP was associated with improvements in subjective reports of sleep quality as measured with a visual analog scale as well as mean sleep latency times on polysomnography.19 Despite the growing body of evidence supporting the use of positive pressure therapy for UARS patients, it remains difficult to obtain therapy. In a follow-up study of more than 90 patients conducted 4 to 5 years after the initial diagnosis of UARS was made, none of the subjects were receiving CPAP treatment; the main rationale given was that their insurance provider declined to provide the necessary equipment.1 Formal follow-up clinical evaluations of these patients noted significant worsening in their sleep-related complaints, with increased reports of fatigue, insomnia, and depressive mood. More disturbingly, prescriptions for hypnotics, stimulants, and antidepressants increased more than fivefold.
Other interventions, such as surgery or oral appliances, have also been used with some success in the treatment of patients with UARS. Procedures such as uvulopalatopharyngoplasty, laser-assisted uvuloplasty (LAUP), septoplasty with turbinate reduction, genioglossus advancement, and radiofrequency ablation of the palate have all been described in the literature.37-40 A study of LAUP in nine patients with UARS who underwent uvulopalatopharyngoplasty (n=2), multilevel pharyngeal surgery (n=1), or LAUP (n=6) reported improvements in subjective daytime sleepiness as measured with Epworth Sleepiness Scale scores.37 In the two patients for whom postoperative polysomnographic data was available, significant improvements in Pes nadir pressures were seen. But patients had several interventions and it is difficult to assess which one was successful. A study of 14 patients with UARS who underwent radiofrequency ablation of the palate also reported improvement in subjective sleepiness, with concurrent improvements in Pes nadir levels and reports of snoring.40 However, prior reviews of the available literature have noted that many of the studies evaluated small numbers of patients, consisted of uncontrolled case reports or series without clear characterization of the subjects enrolled, and had no consistent end points for an adequate evaluation of efficacy.39 Further investigation is required to determine the specific role for surgical intervention in these patients. Other authors have also reported successful treatment of UARS with use of oral appliances, although these studies suffer from the same limitations as the surgical literature.41 In children, orthodontic approaches, such as maxillary distraction or use of expanders, have also shown promising results.

Check this about Flow Limitation (consisting of RERAs and UARs):
A source for a link:
http://www.apneaboard.com/forums/Thread ... e-Syndrome
Do you have Upper Airway Resistance Syndrome (UARS)?
Clinical Features
Patients with UARS have symptoms similar to those seen in OSAS, although there are some distinct features. Much of the research performed has attempted to identify and describe a group of patients with significant daytime sleepiness and disrupted sleep, but without the other dominant clinical features seen in OSAS. Typical symptoms reported by patients with UARS include excessive daytime sleepiness, fatigue, difficulty concentrating, morning headaches, and unrefreshing sleep. There can be also be a significant impairment in daytime functioning; a recent study demonstrated that subjects with UARS performed worse than patients with obstructive sleep apnea hypopnea syndrome and normal control individuals on different aspects of the Psychomotor Vigilance Task. In a separate study, upwards of 30% of subjects with UARS had abnormal sleep-onset latency on the Maintenance of Wakefulness Test. Individuals with abnormal airway anatomy are at increased risk, including those with a decreased retrolingual space, narrow nasal passages, or a small neck circumference. Patients are typically not obese, with a mean BMI often <25 kg/m. They are also usually younger than those in whom OSAS is diagnosed, with a mean age of approximately 38 years. Snoring is not a requisite symptom, with 10% to 15% or more of patients having never or only intermittently snored.
Patients with UARS are also more likely to report symptoms of frequent nocturnal awakening with difficulty falling back to sleep. This is thought to be a potential reason for increased complaints of insomnia amongst patients with UARS, including sleep onset and sleep maintenance problems. In addition to difficulties with acute insomnia, patients with UARS also have an increased likelihood of carrying a diagnosis of chronic insomnia. Other notable complaints include parasomnias, especially sleepwalking, sleep talking, and sleep terrors. Patients may also have symptoms of abnormal autonomic function, including lightheadedness or dizziness on rising from a supine or sitting position, cold hands and feet, and low resting blood pressures (defined as a systolic BP <105 mm Hg with a diastolic BP <65 mm Hg). In a study of 400 patients with UARS, more than 20% met criteria for low BP, a significantly higher prevalence when compared with people who have OSAS (0.6%) or insomnia (0.9%). Interestingly, all subjects in the study had evidence of a small oral cavity on examination with a narrowed airway space dimension on cephalometric radiographs, consistent with other reports. Lastly, patients with UARS have increased rates of symptoms such as gastroesophageal reflux, muscular pain, diarrhea, abdominal pain, depression, and anxiety. This has led some authors to suggest a link between UARS and functional somatic syndromes, such as irritable bowel syndrome, chronic fatigue syndrome, and fibromyalgia. In a study of 75 subjects equally divided into three groups (UARS, mild to moderate OSAS, and severe OSAS), those with UARS were more likely to report symptoms of headache, irritable bowel symptoms, and sleep-initiation insomnia. Subjects with UARS were also more likely to have alpha intrusion during slow-wave sleep, a polysomnographic finding described in a number of fatigue syndromes. In children with UARS, symptoms consistent with attention deficit disorder or attention deficit hyperactivity disorder may be present, with behavioral changes leading to poor school performance.
________________________________________
Clinical Features Associated With UARS
Daytime symptoms:
Excessive daytime sleepiness
Fatigue
Morning headaches
Myalgia’s [muscle pain]
Difficulty concentrating
Sleep disturbances:
Frequent nocturnal awakenings
Difficulties initiating sleep
Insomnia
Bruxism [teeth clenching]
Restless leg syndrome
Unrefreshing sleep
Autonomic nervous system:
Hypotension
Orthostasis [maintenance of an upright standing posture]
Cold hands and feet
Functional somatic syndrome associations:
Depression
Anxiety
Chronic fatigue syndrome
Irritable bowel syndrome
Fibromyalgia
Polysomnographic abnormalities Increased RERAs:
Increased nocturnal arousals
Increased CAP rate [cyclical alternating pattern in EEG]
Alpha intrusion during sleep
Treatment
The optimal treatment for patients with UARS is not currently known. Continuous positive airway pressure (CPAP) has been quite useful in the treatment of sleep-disordered breathing and there are some notable positive results in CPAP treatment of UARS. In a study of 15 heavy snorers with clinical evidence of UARS, treatment with nasal CPAP was associated with decreases in observed nocturnal arousals on polysomnography and decreases in mean sleep latency times on multiple sleep latency testing (MSLT) after several nights of treatment. A follow-up study of 15 subjects (in the original description of UARS) with daytime sleepiness and fatigue and who had undergone a therapeutic trial of positive pressure therapy reported similar findings. After treatment with approximately a month of nasal CPAP, significant improvements were seen in mean sleep latency times on MSLT (5.3 minutes vs 13.5 minutes), Pes nadir pressure (–33.1 cm H2O vs –5.3 cm H2O), amount of slow-wave sleep (1.2% vs 9.7%), and EEG arousals (31.3 vs 7.9 events/hour of sleep). Along with an improvement in sleep latency times on MSLT, there were subjective reports of improved daytime symptoms. Lastly, in a study of 130 postmenopausal women with chronic insomnia and evidence of UARS (n=62) or normal breathing (n=68), treatment with either nasal turbinectomy or nasal CPAP was associated with improvements in subjective reports of sleep quality as measured with a visual analog scale as well as mean sleep latency times on polysomnography.19 Despite the growing body of evidence supporting the use of positive pressure therapy for UARS patients, it remains difficult to obtain therapy. In a follow-up study of more than 90 patients conducted 4 to 5 years after the initial diagnosis of UARS was made, none of the subjects were receiving CPAP treatment; the main rationale given was that their insurance provider declined to provide the necessary equipment.1 Formal follow-up clinical evaluations of these patients noted significant worsening in their sleep-related complaints, with increased reports of fatigue, insomnia, and depressive mood. More disturbingly, prescriptions for hypnotics, stimulants, and antidepressants increased more than fivefold.
Other interventions, such as surgery or oral appliances, have also been used with some success in the treatment of patients with UARS. Procedures such as uvulopalatopharyngoplasty, laser-assisted uvuloplasty (LAUP), septoplasty with turbinate reduction, genioglossus advancement, and radiofrequency ablation of the palate have all been described in the literature.37-40 A study of LAUP in nine patients with UARS who underwent uvulopalatopharyngoplasty (n=2), multilevel pharyngeal surgery (n=1), or LAUP (n=6) reported improvements in subjective daytime sleepiness as measured with Epworth Sleepiness Scale scores.37 In the two patients for whom postoperative polysomnographic data was available, significant improvements in Pes nadir pressures were seen. But patients had several interventions and it is difficult to assess which one was successful. A study of 14 patients with UARS who underwent radiofrequency ablation of the palate also reported improvement in subjective sleepiness, with concurrent improvements in Pes nadir levels and reports of snoring.40 However, prior reviews of the available literature have noted that many of the studies evaluated small numbers of patients, consisted of uncontrolled case reports or series without clear characterization of the subjects enrolled, and had no consistent end points for an adequate evaluation of efficacy.39 Further investigation is required to determine the specific role for surgical intervention in these patients. Other authors have also reported successful treatment of UARS with use of oral appliances, although these studies suffer from the same limitations as the surgical literature.41 In children, orthodontic approaches, such as maxillary distraction or use of expanders, have also shown promising results.
_________________
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: S9 Autoset machine; Ruby chinstrap under the mask straps; ResScan 5.6 |
Last edited by avi123 on Mon Jul 01, 2013 10:01 am, edited 3 times in total.
Re: 0.0
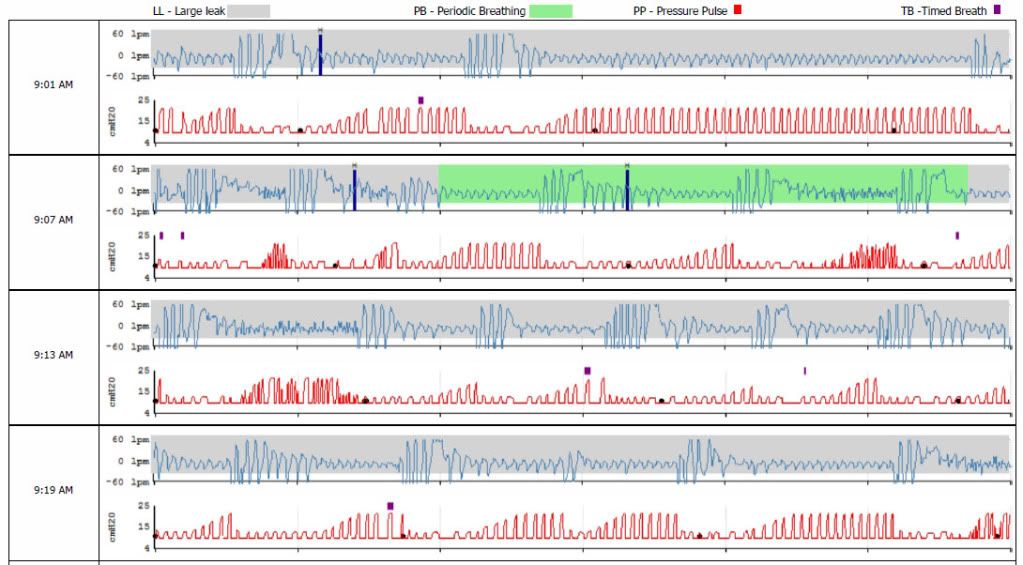
Thanks for your interest, DreamDiver. Sure, here's the zoomed in 5-minute view of the three hold-breath (over 10 seconds) tests I did with Flow Rate graph just below it. No, my tongue was not back blocking my throat shut. As can be seen here, no attempt is made by ResMed to hide these apneas, which I think would probably be graphed as Centrals IF centrals were graphically distinguished from Obstructives in Adapt graphs.DreamDiver wrote:Did you hold your breath with your throat closed or with your throat open? Could you zoom in at a five minute window on just the shorter of the two example apneas giving the flow graph just below the event graph?Papit wrote:... A few minutes before turning off my machine on 6/27, I held my breath three times that I guesstimated were for 15, 25, and 35 seconds. ...

Note that I had to use SH to see the Flow Rate graph. Although I see "Flow" (in addition to "Flow Limitation" and the usual graphs) listed under Tools>Options>Preferences>Detailed Graphs>Graphs, no "Flow" graph comes up for me except "Flow Limitation". Curious, but possibly explainable by the unit's more recent manufacture as I received it only two weeks ago. Maybe they tweaked something. Anybody have a tech support number for the company?
_________________
| Mask: DreamWear Nasal CPAP Mask with Headgear |
| Additional Comments: Machine: AirCurve 10 ASV (37043), Software:ResScan 5.7.0.9477, SleepyHead V1.00BETA2, Oximeter:CMS-50i |
Last edited by Papit on Sun Jun 30, 2013 7:36 pm, edited 1 time in total.
Machine: AirCurve 10 ASV, Mask: AirFit N30i
PulseOx Data-transfer to OSCAR4-23-12http://tinyurl.com/nzd64gu
Wireless SD Card Data-transfer to OSCAR 8-14-15http://tiny.cc/z1kv8x
PulseOx Data-transfer to OSCAR4-23-12http://tinyurl.com/nzd64gu
Wireless SD Card Data-transfer to OSCAR 8-14-15http://tiny.cc/z1kv8x
-
DreamDiver
- Posts: 3082
- Joined: Thu Oct 04, 2007 11:19 am
Re: 0.0
Did you hold your breath with your throat closed or with your throat open? Could you zoom in at a five minute window on just the shorter of the two example apneas giving the flow graph just below the event graph?Papit wrote:... A few minutes before turning off my machine on 6/27, I held my breath three times that I guesstimated were for 15, 25, and 35 seconds. ...
_________________
| Mask: ResMed AirFit™ F20 Mask with Headgear + 2 Replacement Cushions |
| Additional Comments: Pressure: APAP 10.4 | 11.8 | Also Quattro FX FF, Simplus FF |
Re: 0.0
Gents, while ResMed does not distinguish between OA and CA in the Adapt reports and graphs (it combines them), it certainly DOES show and report them. I did my own test. A few minutes before turning off my machine on 6/27, I held my breath three times that I guesstimated were for 15, 25, and 35 seconds. See charts below. Notice how promptly the machine elevates its pressure to push air into me and treat for the three (intentional) halts in my air flow. (Re. the ongoing discussion about the quirky appearance of a Flow Limitation graph for an Adapt machine, notice that no flow limitations appear on the graph in sync with my three extended halts in breath.)DreamDiver wrote:Technically, we should be able to do it by looking carefully at the graphs. CA's are fairly easy to spot in a 10-minute window or 5-minute window, confirmable in a minute/thirty-second window.avi123 wrote:... Resmed would not let CAs to show, untreated, from a machine that was designed to eliminate them. To check the reliability of those Resmed VPAP Adapt ASV machines you need a third party to do it. Something like the Consumer Reports but for CPAP users.

_________________
| Mask: DreamWear Nasal CPAP Mask with Headgear |
| Additional Comments: Machine: AirCurve 10 ASV (37043), Software:ResScan 5.7.0.9477, SleepyHead V1.00BETA2, Oximeter:CMS-50i |
Machine: AirCurve 10 ASV, Mask: AirFit N30i
PulseOx Data-transfer to OSCAR4-23-12http://tinyurl.com/nzd64gu
Wireless SD Card Data-transfer to OSCAR 8-14-15http://tiny.cc/z1kv8x
PulseOx Data-transfer to OSCAR4-23-12http://tinyurl.com/nzd64gu
Wireless SD Card Data-transfer to OSCAR 8-14-15http://tiny.cc/z1kv8x
Re: 0.0
That's funny, Avi. Actually I'm under 5' 10" and weigh 165 so no need to keep your distance!avi123 wrote:Papit, thanks for showing the above Stats. If you feel good then it is all that's count.
Your Tidal Volume indicates that you're physically a larger person then I am. You are
taller than 6' 2" and weigh more than 220 lb. So I stay away from you
In above link given by DD post I see this by Nate for his VPAP Adapt ASV:
NO CENTRALS ARE SHOWN . . .
Re. Centrals data on my graphs and reports, there are none shown. Centrals and Obstructives are combined and shown as AI. My graphs (except for the appearance of Flow Limitations), data, reports, and machine are exactly like Nate's. I wish they broke out CA and OA as they do on the AutoSet as viewed in ResScan and SH, but the machine keeps my total AHI under 5 almost every day, usually well under 5, so I'm a happy camper.
_________________
| Mask: DreamWear Nasal CPAP Mask with Headgear |
| Additional Comments: Machine: AirCurve 10 ASV (37043), Software:ResScan 5.7.0.9477, SleepyHead V1.00BETA2, Oximeter:CMS-50i |
Last edited by Papit on Sat Jul 06, 2013 9:58 pm, edited 1 time in total.
Machine: AirCurve 10 ASV, Mask: AirFit N30i
PulseOx Data-transfer to OSCAR4-23-12http://tinyurl.com/nzd64gu
Wireless SD Card Data-transfer to OSCAR 8-14-15http://tiny.cc/z1kv8x
PulseOx Data-transfer to OSCAR4-23-12http://tinyurl.com/nzd64gu
Wireless SD Card Data-transfer to OSCAR 8-14-15http://tiny.cc/z1kv8x
-
DreamDiver
- Posts: 3082
- Joined: Thu Oct 04, 2007 11:19 am
Re: 0.0
Technically, we should be able to do it by looking carefully at the graphs. CA's are fairly easy to spot in a 10-minute window or 5-minute window, confirmable in a minute/thirty-second window.avi123 wrote:... Resmed would not let CAs to show, untreated, from a machine that was designed to eliminate them. To check the reliability of those Resmed VPAP Adapt ASV machines you need a third party to do it. Something like the Consumer Reports but for CPAP users.
_________________
| Mask: ResMed AirFit™ F20 Mask with Headgear + 2 Replacement Cushions |
| Additional Comments: Pressure: APAP 10.4 | 11.8 | Also Quattro FX FF, Simplus FF |
Re: 0.0
[quote="JohnBFisher
So what this means is that the CAI is always zero on an ASV machine or its not working properly. If the neural drive slows down to pause >10s the machine will automatically insert a breath before the end of that time period before you have a chance to test the airway for being open or closed. If it fails to create flow, it was obstructive.
[/quote] (My emphasis on the last part.)
Well, that might be the Resmed Spokesman's definition of no central apnea, but if you have serious enough problems, a central apnea WILL occur. I offer my own example. This was from a PR System One ASV unit, which does not pretend that no central apnea occurs.
Comment,
Well, that's what I been saying all along, that Resmed would not let CAs to show, untreated, from a machine that was designed to eliminate them. To check the reliability of those Resmed VPAP Adapt ASV machines you need a third party to do it. Something like the Consumer Reports but for CPAP users.
So what this means is that the CAI is always zero on an ASV machine or its not working properly. If the neural drive slows down to pause >10s the machine will automatically insert a breath before the end of that time period before you have a chance to test the airway for being open or closed. If it fails to create flow, it was obstructive.
[/quote] (My emphasis on the last part.)
Well, that might be the Resmed Spokesman's definition of no central apnea, but if you have serious enough problems, a central apnea WILL occur. I offer my own example. This was from a PR System One ASV unit, which does not pretend that no central apnea occurs.
Comment,
Well, that's what I been saying all along, that Resmed would not let CAs to show, untreated, from a machine that was designed to eliminate them. To check the reliability of those Resmed VPAP Adapt ASV machines you need a third party to do it. Something like the Consumer Reports but for CPAP users.
_________________
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: S9 Autoset machine; Ruby chinstrap under the mask straps; ResScan 5.6 |
-
DreamDiver
- Posts: 3082
- Joined: Thu Oct 04, 2007 11:19 am
Re: 0.0
JohnBFisher, I am unfamiliar with some of the stuff I'm seeing on the PR graph you provided. Excluding wave forms, which ticks/markings depict centrals? Also, am I right in seeing that you have large leak all the way through? Is the quattro fx comfortable on the nose bridge for you?JohnBFisher wrote:...
Well, that might be the Resmed Spokesman's definition of no central apnea, but if you have serious enough problems, a central apnea WILL occur. I offer my own example. This was from a PR System One ASV unit, which does not pretend that no central apnea occurs.
IMAGE
Sure, even when I stopped breathing there was some air movement because the unit quickly ramped up the air pressure. But the point is that my body was not responsible for that. I was in the middle of a series of central apneas.
_________________
| Mask: ResMed AirFit™ F20 Mask with Headgear + 2 Replacement Cushions |
| Additional Comments: Pressure: APAP 10.4 | 11.8 | Also Quattro FX FF, Simplus FF |
Re: 0.0
Congrats!
-
JohnBFisher

- Posts: 3821
- Joined: Wed Oct 14, 2009 6:33 am
Re: 0.0
Well, that might be the Resmed Spokesman's definition of no central apnea, but if you have serious enough problems, a central apnea WILL occur. I offer my own example. This was from a PR System One ASV unit, which does not pretend that no central apnea occurs.DreamDiver wrote:It's not that the ASV doesn't detect them - it's supposed to prevent them altogether by recognizing signs and increasing SV as necessary or the machine isn't working properly.(My emphasis on the last part.)Resmed Spokesperson wrote:- The definition of an apnea is a cessation of breathing for greater than 10s, meaning a person's natural breathing rate would have to be slower than <6 breaths per minute for the airway to stay open naturally. This is important due to the back up rate settings
- A servo ventilator treats compSA and CSA by adding in breath support when the central drive slows down below the natural breath rate. i.e. it starts to breathe for you, when you brain starts to slow down.
- If the device inserts a breath and is unable to create flow, the airway is blocked, or an obstructive apnea.
So what this means is that the CAI is always zero on an ASV machine or its not working properly. If the neural drive slows down to pause >10s the machine will automatically insert a breath before the end of that time period before you have a chance to test the airway for being open or closed. If it fails to create flow, it was obstructive.
Here's a video from this page.
Sure, even when I stopped breathing there was some air movement because the unit quickly ramped up the air pressure. But the point is that my body was not responsible for that. I was in the middle of a series of central apneas.
_________________
| Mask: Quattro™ FX Full Face CPAP Mask with Headgear |
| Additional Comments: User of xPAP therapy for over 20 yrs. Resmed & Respironics ASV units with EEP=9cm-14cm H2O; PSmin=4cm H2O; PSmax=15cm H2O; Max=25cm H2O |
"I get up. I walk. I fall down. Meanwhile, I keep dancing” from Rabbi Hillel
"I wish to paint in such a manner as if I were photographing dreams." from Zdzisław Beksiński
"I wish to paint in such a manner as if I were photographing dreams." from Zdzisław Beksiński