NotMuffy wrote:there is also the preaforementioned issue of the breathing irregularity of phasic REM. And I think that as the REM-suppressant medication effect wears off in the latter part of the night, you have a pile of it (that might be an interesting thing to look for in your raw NPSG data).
Okay, I am interested in interesting. And actually, I want the data because making unexpected requests of my medical care providers is, in and of itself, interesting. When I call the sleep lab to ask for the raw NPSG data, what exactly do I ask for?
NotMuffy wrote:You probably want to leave the variability of phasic REM alone (including centrals that are in there. They are generally considered to be normal phenomenon.)
Okay. So, any irregularities during phasic REM, I can cross off the list of Events About Which I Shall Be Concerned.
Also cross off that list Any Central Apnea Events Occurring After A Sigh.
NotMuffy wrote:the coarseness of that pressure channel makes everything look like a PP.
I don't understand what that means.
In this area:
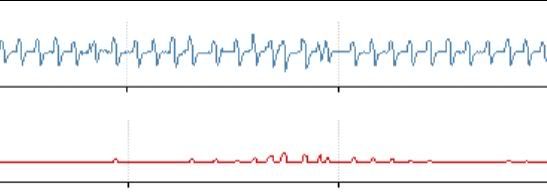
NotMuffy wrote:breathing looks a little irregular, but that's about it. Because of its location, it could be REM, and the algorithm has opted to bang on it with some IPAP. Was the first one justified by some FL characteristic? The response Is a breath late, and anyway, it just looks a little noisy to me, and perhaps artifactual.
The waves of my breathing look a little noisy? Artifactual as in maybe I was turning over or something, causing irregular breathing? I have some questions about making sense of the waves, including how to see that the response to the first one was a breath late, but I will save those for a later post, once I have a chance to cut out some of the other areas I had questions about.
NotMuffy wrote:The last couple of DLs with AHI 9.0 - 10.1 are certainly a vast improvement over the 19.0 - 36.0.
Yes, those are much better numbers. Still not great, but better.
NotMuffy wrote:I think it's very important to keep in mind the priorly preaforementioned points-- that because of at least 3 factors, your underlying sleep architecture is probably fragmented. Not horrifically so, but I think you're drifting over and under the 100 arousals/night threshold that tends to predict the incidence of EDS
Three factors... Medication and... and... Oh, *#@%(!! I can only remember one of them!! (Yes, I will wash my hands off with soap before I eat!)
To somewhat paraphrase NotMuffy---
If, after all the dial wingin', there's still evidence of underlying sleep fragmentation, then the next steps would be to optimize the factors that affect sleep continuity, by addressing medication issues, along with addressing two other priorly and previously preaforementioned issues, which have been forgotten by Paper_Nanny. Is that an accurate paraphrasement? No change in the meaning, only change in the wording?
NotMuffy wrote:For instance, sitting down with a sharp pharmacist and looking at drug hygiene may be helpful (if that hasn't already been done). Stuff like looking at nighttime duloxetine dose and seeing if that's the best way to meet goal (does the lowering of arousal threshold create more issues than amelioration of other symptoms). Or if anything can be done with the methylphenidate - modafinil thing.
Who was it who said in an earlier post that the word hygiene reminded him of junior high health class? Was it Mr. Bill? And did I totally mangle the specifics of what was said? I have bad associations with that word, tool. Sixth grade sex education, separate classes for the boys and the girls. The boys got to learn interesting things about human reproduction. The girls got to learn about menstrual hygiene. Because of that, the word hygiene has traces of sexual discrimination attached to it in my mind. Why didn't the girls get to learn both about human reproduction
and about menstrual hygiene?? Working in group homes for people with developmental disabilities. Endless hygiene goals for the people living in the homes. One of the staff members I supervised
loved the word hygiene. I associate the word with her and feel somewhat nauseated. Hygienics is a slightly more palatable form of the word. Interestingly enough, her second favourite word was menses.
Possibly I can sit down with a sharp pharmacist. I
think Holly at my usual pharmacy is sharp, but maybe I have misjudged her. I can ask her if there is a time we can sit down and review my drug list. Specifically, I will be asking her-- Which medications are causing sleep fragmentation? Would it make a difference if I changed the times on those medications? (eg take my second dose of duloxetine earlier in the day) Are there medications that do the same thing without causing sleep fragmentation?
What is the issue with the methylphenidate- modafinil thing? I wonder how much of my need for prescription amphetamines and other Keep Me Awake drugs is a question of which came first, the music or the misery, as Fall Out Boy would put it.
NotMuffy wrote:Of course, drug wingin' certainly has it's risks. An abrupt baclofen - duloxetine discontinuance would undoubtedly result in something that looks like the final scene in Total Recall (I know you know that, but I'll bet more than a few others don't).
I will take the restraints off if you
promise not to hit me!!
Deborah










