Muffy wrote: Well this algorithm is certainly working out well:
...
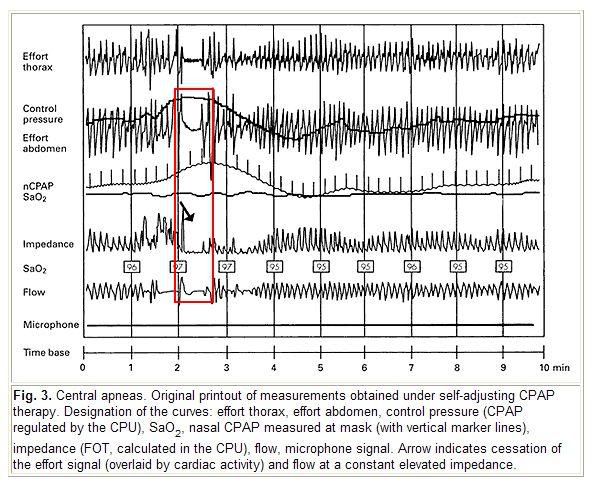
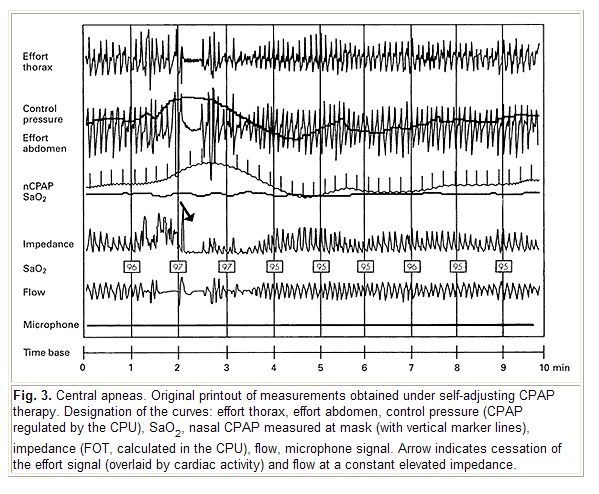
CPAP pressure is merrily increasing...
Well, I observe this detection/response sequence in that graph above: 1) pressure increases in response to high airway resistance only after flow also drops, 2)
then FOT suddenly detects an airway impedance drop, 3) thus the CPAP pressure no longer increases---but instead performs a very gradual pressure drop. By my take the FOT algorithm is administering the correct pressure response just as soon as airway impedance plummets along with that low flow.
And I believe the authors are citing that graph as a correct algorithmic response based on those same FOT-detected impedance variations as well.
Muffy wrote:Right. But here is an example presented to illustrate the subroutine:
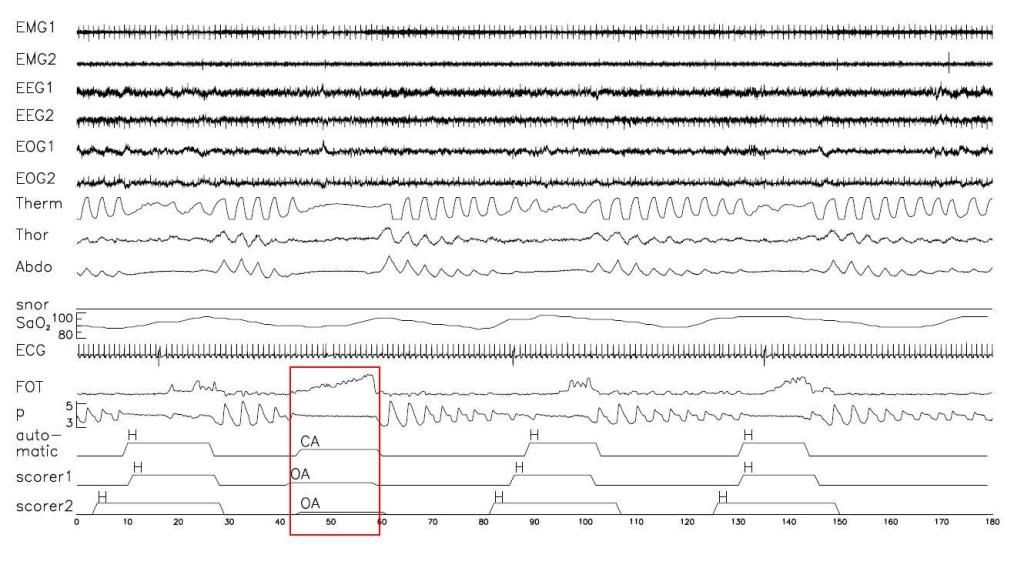
Thanks for demonstrating with that graph... So it's really not all that crazy after all...
And in general it makes
good sense that any one high-specificity detection routine can nicely supplement another high-specificity routine that happens to entail non-congruent sensitivity---assuming you have the real-time CPU cycles to dole out. Where one routine missed detection based on lacking sensitivity, the other routine can nicely pick up some margin of those missed events. While that adjunct approach boosts detection sensitivity, that's not to say its guaranteed to lend perfect or even near-perfect detection sensitivity.
Muffy wrote:but the subroutine identified cardiac oscillations in the FOT channel (while the airway is CLOSING?)
Well, we might want to revisit those contending theories about cardiac pulsations being more detectable for reasons
other than open-airway wave-guiding. I'll see if I can dig them up for more techno-weenie chit-chat fun tomorrow...














{kind=link}